Downloaded 61 times
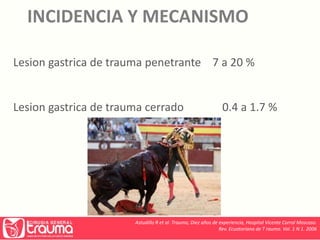



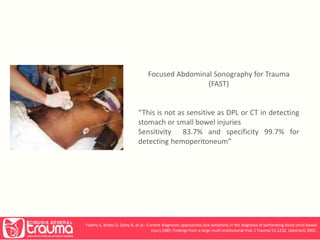
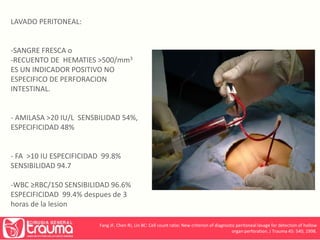

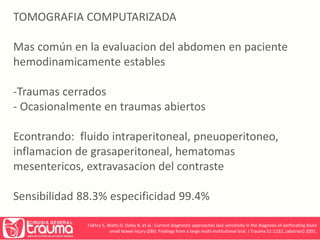
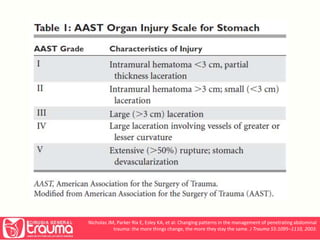
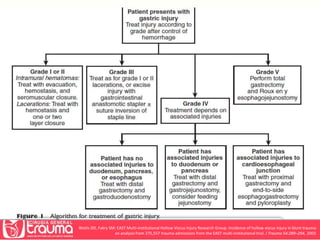
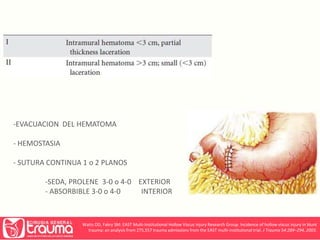
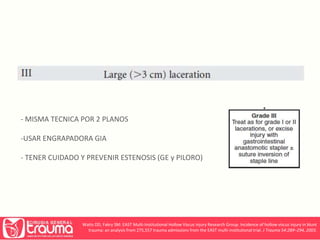
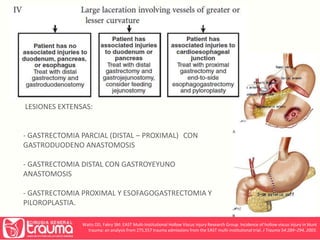

This document discusses trauma to the esophagus and stomach. It provides information on the incidence, mechanisms, diagnosis and management of injuries to these areas. It notes that esophageal injuries are rare, usually due to penetrating injuries to the neck. Diagnosis involves considering mechanism of injury and symptoms like dysphonia. Tests include swallowing contrast and endoscopy. Management involves controlling leaks, debridement and drainage. Surgical repair depends on location and can include primary closure or esophagostomy. For stomach injuries, it discusses history and signs/symptoms. Diagnostic tests include lavage, ultrasound, CT scan and laparoscopy. Surgical management involves evacuation, hemostasis and suturing perforations, with resection