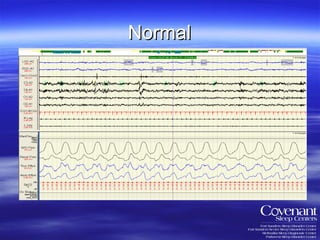
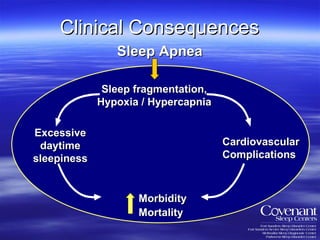
1. The document discusses sleep, sleep disorders like sleep apnea, and how sleep changes with age. It covers the definition of sleep, sleep stages, consequences of sleep deprivation, and prevalence of sleep disorders.
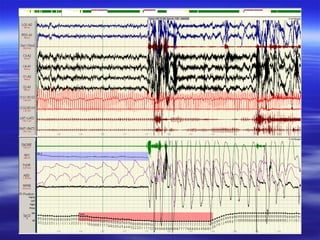
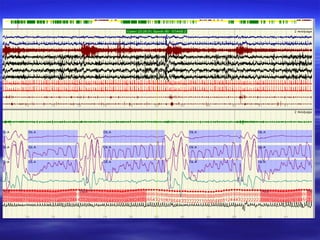
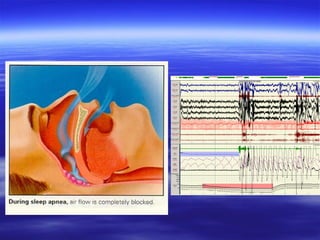
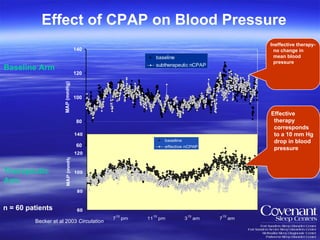
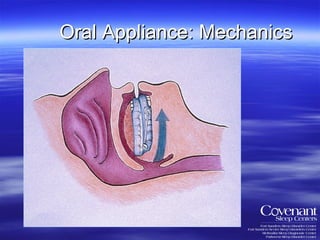
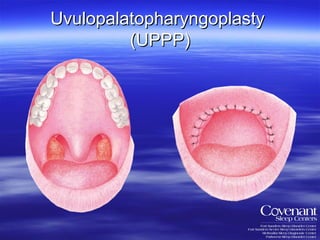
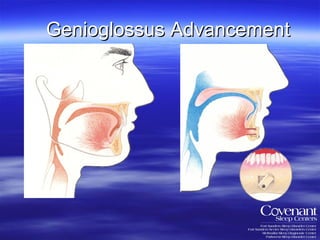
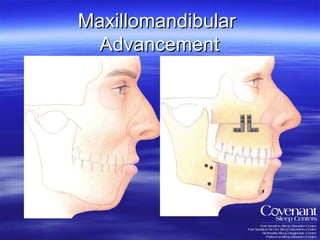
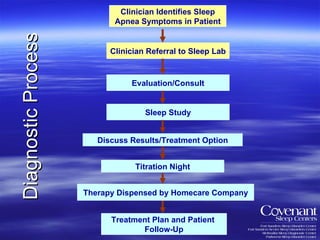
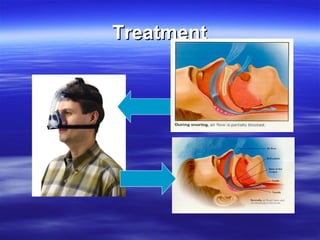
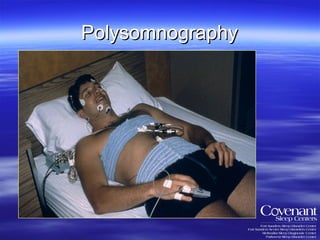
2. Treatment options for sleep apnea are discussed, including CPAP, oral appliances, and surgery. Diagnosis involves a sleep study.
3. Sleep changes as people age, with less deep sleep and more nighttime awakenings. Medical conditions can also affect older adults' sleep. Seeking help from a sleep specialist is recommended for persistent sleep issues.