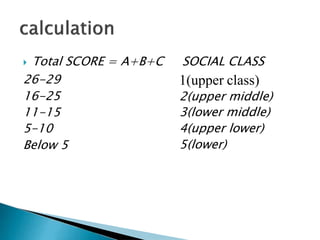
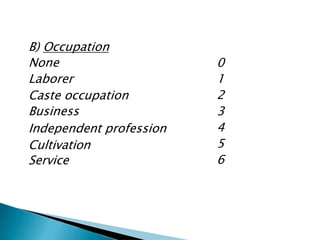
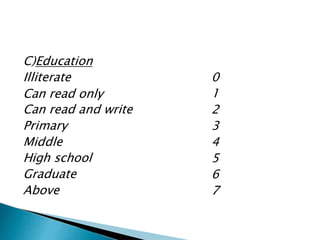
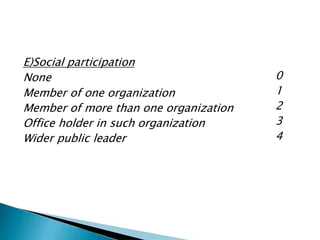
This document provides an overview of socioeconomic status (SES) and methods used to determine it. It defines SES and discusses its importance in health research. Major factors that affect SES include education, occupation, and income. Several scales are used to measure SES, including the Modified Kuppuswamy Scale, Modified BG Prasad Classification, and the Standard of Living Index. Appropriate scales depend on whether the setting is urban or rural. The document also provides sample questions to assess SES and limitations of different scales.


























![MCQs
Modified Kuppuswamy scale include all criteria for
socioeconomic status except: [AIPGME ]
(a) Income of family per month
(b) Education of head of family
(c) Occupation of head
(d) Income of Family Head
Ans.D](https://image.slidesharecdn.com/socioeconomicstatusdetermination-180314060335/85/Socioeconomic-status-determination-47-320.jpg)