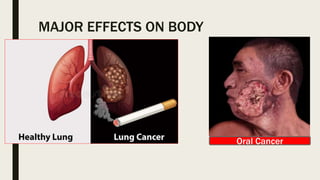
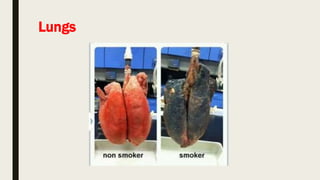
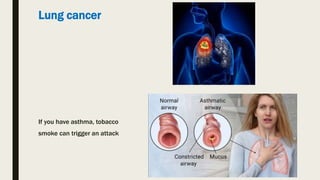
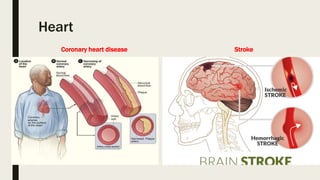
This document discusses the harmful health effects of smoking and tobacco use, including increased risk of various cancers and respiratory and cardiovascular diseases. It also outlines initiatives by the Indian government to educate the public and implement policies and programs to prevent tobacco use and encourage smoking cessation. Recommendations include school health programs, media campaigns, establishing tobacco cessation centers, training health workers, and utilizing dental practitioners to educate patients and discourage tobacco use.






![Lung Diseases
COPD [Chronic Obstructive Pulmonary Disease]](https://image.slidesharecdn.com/8ca1pww7rpsybgp48epn-signature-d342e2cf86652cd0b6260b069001d2da88c816d7a632b18f4f81976a52a3f92f-poli-190915081529/85/Smoking-patient-education-16-320.jpg)

























































![TOBACCO NATIONAL TOBACCO CONTROL PROGRAMME [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/tobaccoautosaved-250922162145-6c1b1cd5-thumbnail.jpg?width=640&height=640&fit=bounds)







































