This document provides information on a presentation about tobacco. Some key points:
- Smoking remains a leading cause of preventable illness and death in Canada. Saskatchewan has high smoking rates, especially among youth.
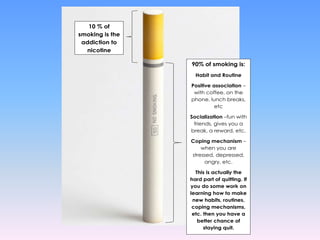
- Secondhand and thirdhand smoke harm others exposed to tobacco smoke. Quitting tobacco can be challenging due to nicotine addiction and behavioral factors.
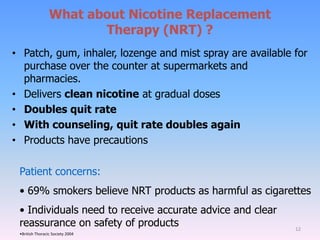
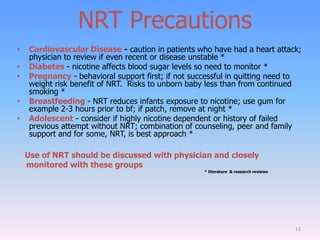
- Healthcare providers should use the 5 A's approach (Ask, Advise, Assess, Assist, Arrange) to counsel patients on quitting smoking. This involves discussing reasons to quit, barriers to quitting, and treatment options like nicotine replacement therapy.
- While some providers may hesitate to counsel patients due to their own smoking status,











































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


















