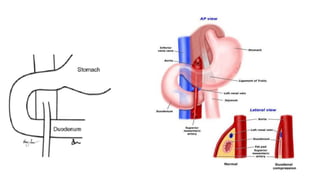
Superior Mesenteric Artery (SMA) syndrome is a rare condition where the third part of the duodenum is compressed between the abdominal aorta and SMA, causing gastric outlet obstruction. It occurs when the angle between the vessels decreases below normal, usually due to weight loss or other factors. Symptoms include early satiety, nausea, vomiting and abdominal pain. Diagnosis involves imaging tests to measure the aortomesenteric angle and distance. Treatment ranges from nutritional support and positioning changes to surgery like duodenojejunostomy to bypass the obstruction. SMA syndrome is difficult to diagnose and treat, but awareness of risk factors and appropriate management can help resolve symptoms.