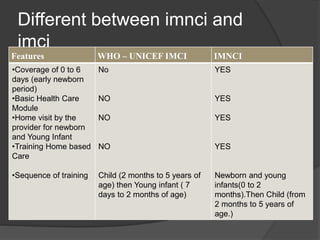
The document discusses Integrated Management of Neonatal and Childhood Illness (IMNCI), an integrated approach to child health that focuses on well-being from birth to 5 years old. IMNCI aims to reduce mortality, illness, and disability in children while promoting growth and development. It includes both preventative and curative elements implemented by families, communities, and health facilities. Key aspects of IMNCI include assessing children for danger signs and illnesses, classifying conditions, treating illnesses, counseling caretakers, and conducting home visits for young infants to promote health. The approach uses standardized case management, focuses on common causes of mortality, and improves health worker skills through evidence-based training.