This document provides an overview of Integrated Management of Neonatal and Childhood Illness (IMNCI). Some key points:
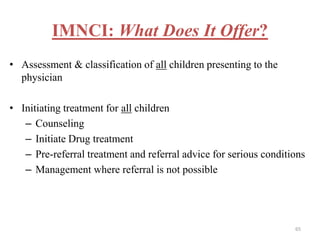
- IMNCI is an integrated approach that aims to reduce death, illness and disability among children under five by improving case management skills, health systems, and family/community health practices.
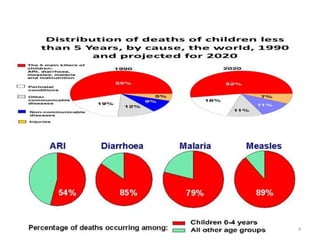
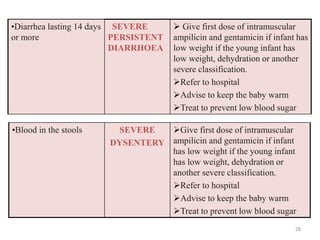
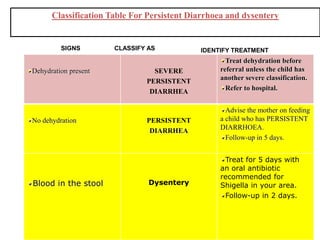
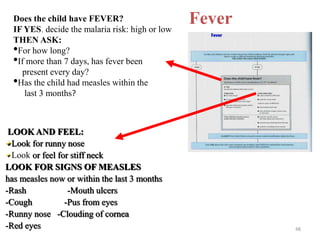
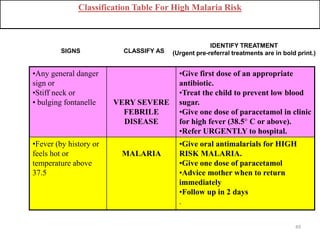
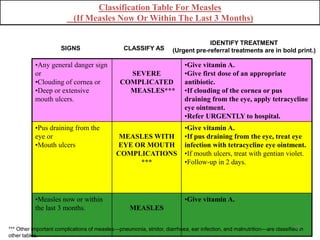
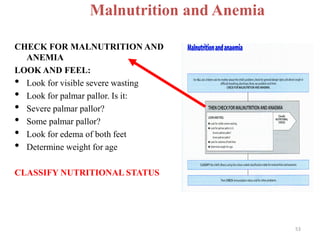
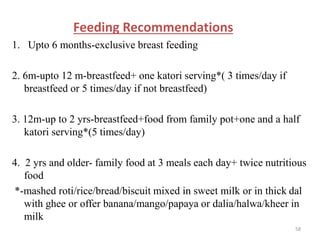
- It focuses on preventing and treating the major causes of childhood mortality like pneumonia, diarrhea, malaria, measles and malnutrition.
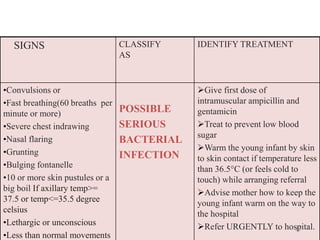
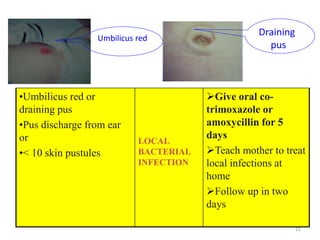
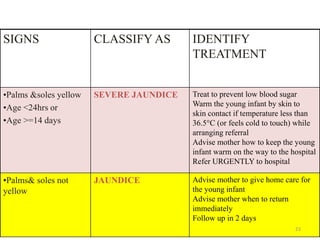
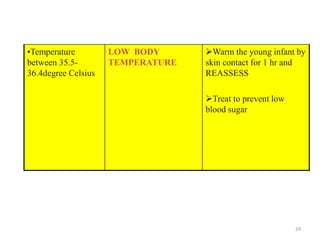
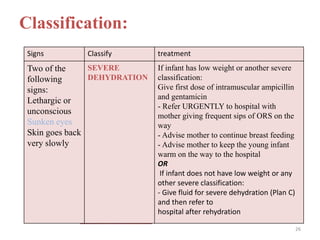
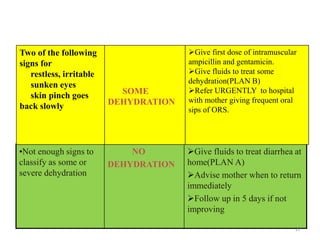
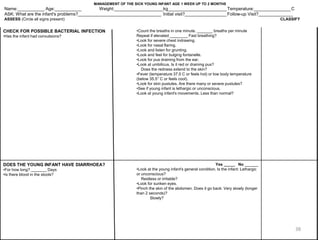
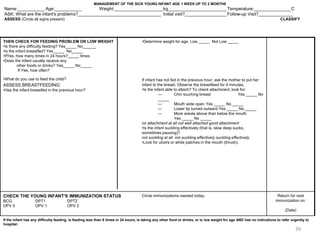
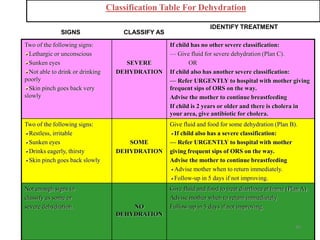
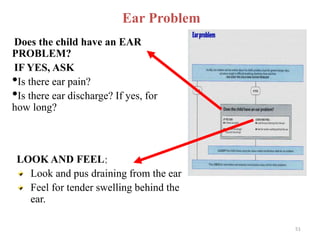
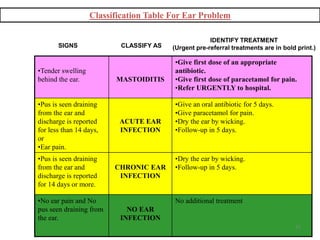
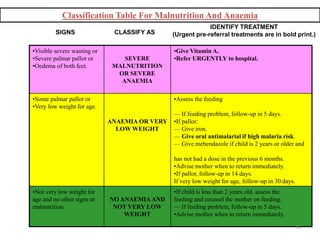
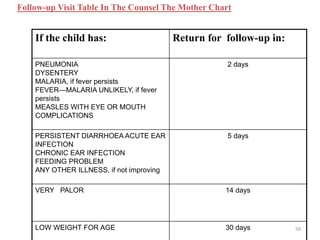
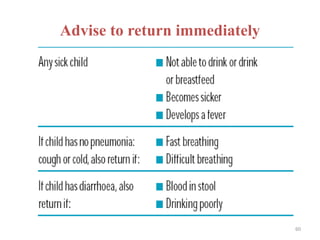
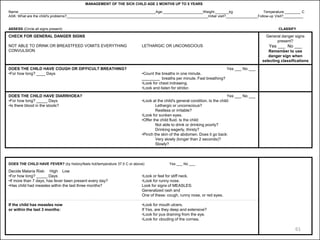
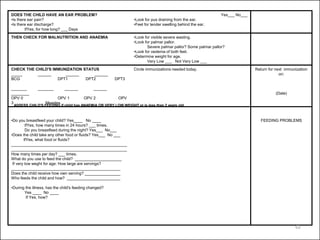
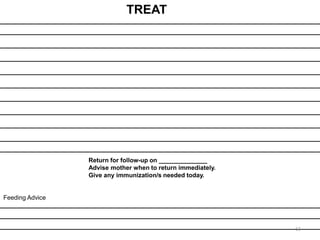
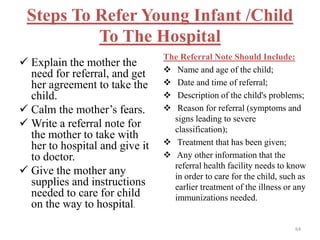
- The case management process involves assessing, classifying, identifying appropriate treatment, counseling the mother, and follow up care for sick young infants and children. Classification is done using a color-coded triage system.
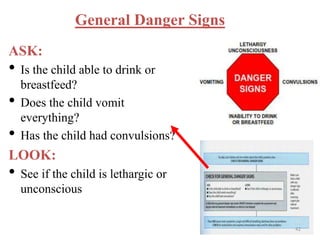
- For young infants, signs like