Why study maturity
indicators?
Keyto successful treatment in
growing
patients – harnessing of growth.
Without exact status of growth –
magnitude and direction-
treatment
planning is futile.
3.
Advantages of Maturity
Indicators
Potentialvector of facial development
determined.
Amount of significant craniofacial
growth
potential left.
To decide the onset of treatment
timing.
Age
Expressed as:
Chronologicage
Age measured by years
lived since birth
Dental age
Determined according
to
teeth erupted, amount of root
resorption
and amount of root formation.
Skeletal age
Determined by ossification
of various skeletal structures at
different
time.
Skeletal Age Assessment
Regions used for skeletal age assessment
should be ideally:
Small to restrict radiation
exposure
Should have many ossification
centres
that ossify at different times and
which
can be standardized
Easily accessible
9.
Regions Normally UsedFor Age
Assessment
Head and neck:
Skull Cervical
vertebrae
Upper limb:
Shoulder joint- scapula
Elbow Hand wrist and
fingers
Hand Wrist Radiographs
Hand wrist – Numerous Small Bones
Predictable and scheduled pattern of
appearance, ossification and union
from
birth to maturity
Most suited to study
growth
12.
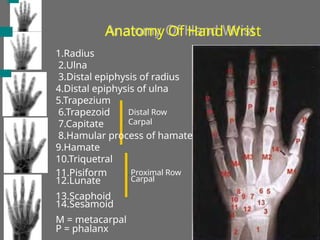
Anatomy Of HandWrist
1.Radius
2.Ulna
3.Distal epiphysis of radius
4.Distal epiphysis of ulna
5.Trapezium
6.Trapezoid
7.Capitate
8.Hamular process of hamate
9.Hamate
10.Triquetral
11.Pisiform
12.Lunate
13.Scaphoid
14.Sesamoid
M = metacarpal
Distal Row
Carpal
Proximal Row
Carpal
P = phalanx
13.
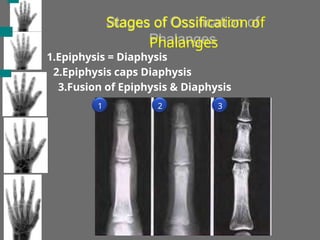
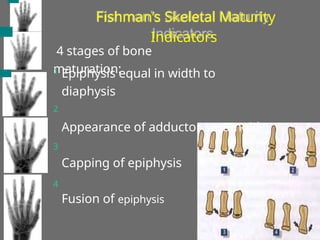
Stages of Ossificationof
Phalanges
1.Epiphysis = Diaphysis
2.Epiphysis caps Diaphysis
3.Fusion of Epiphysis & Diaphysis
1 2 3
14.
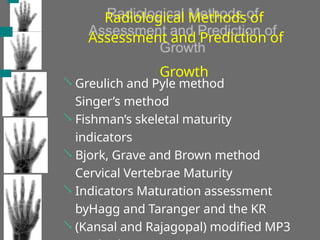
Radiological Methods of
Assessmentand Prediction of
Growth
Greulich and Pyle method
Singer’s method
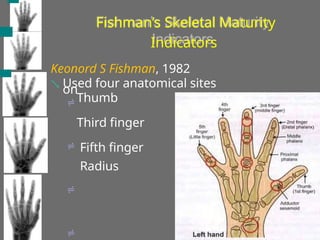
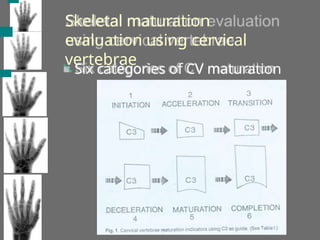
Fishman’s skeletal maturity
indicators
Bjork, Grave and Brown method
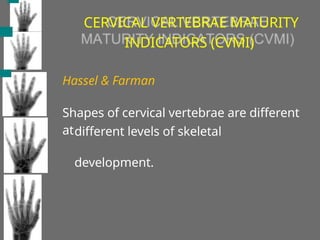
Cervical Vertebrae Maturity
Indicators Maturation assessment
byHagg and Taranger and the KR
(Kansal and Rajagopal) modified MP3
15.
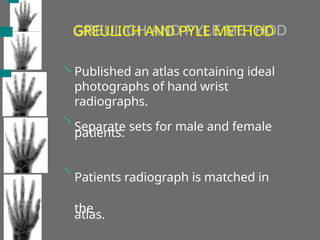
GREULICH AND PYLEMETHOD
Published an atlas containing ideal
photographs of hand wrist
radiographs.
Separate sets for male and female
patients.
Patients radiograph is matched in
the
atlas.
16.
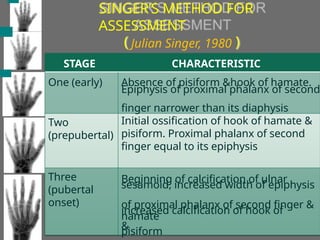
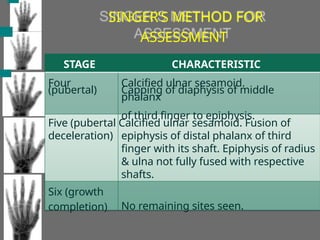
SINGER’S METHOD FOR
ASSESSMENT
JulianSinger, 1980
( )
Three
(pubertal
onset)
STAGE
One (early)
Two
(prepubertal)
CHARACTERISTIC
Absence of pisiform &hook of hamate.
Epiphysis of proximal phalanx of second
finger narrower than its diaphysis
Initial ossification of hook of hamate &
pisiform. Proximal phalanx of second
finger equal to its epiphysis
Beginning of calcification of ulnar
sesamoid, increased width of epiphysis
of proximal phalanx of second finger &
increased calcification of hook of
hamate
&
pisiform
17.
STAGE CHARACTERISTIC
Four
(pubertal)
Calcified ulnarsesamoid.
Capping of diaphysis of middle
phalanx
of third finger to epiphysis.
Five (pubertal Calcified ulnar sesamoid. Fusion of
deceleration) epiphysis of distal phalanx of third
finger with its shaft. Epiphysis of radius
& ulna not fully fused with respective
shafts.
No remaining sites seen.
Six (growth
completion)
SINGER’S METHOD FOR
ASSESSMENT
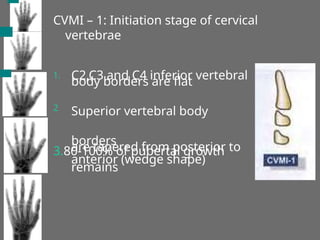
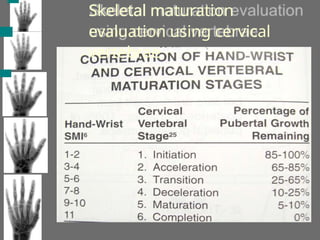
CVMI – 1:Initiation stage of cervical
vertebrae
1. C2,C3 and C4 inferior vertebral
body borders are flat
Superior vertebral body
borders
are tapered from posterior to
anterior (wedge shape)
2
3.80-100% of pubertal growth
remains
24.
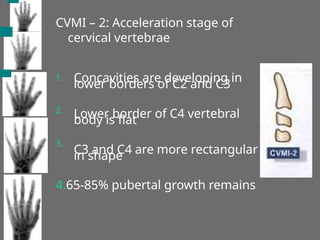
CVMI – 2:Acceleration stage of
cervical vertebrae
1. Concavities are developing in
lower borders of C2 and C3
Lower border of C4 vertebral
body is flat
C3 and C4 are more rectangular
in shape
2.
3.
4.65-85% pubertal growth remains
25.
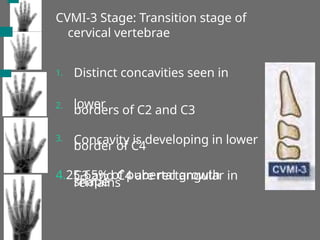
CVMI-3 Stage: Transitionstage of
cervical vertebrae
1. Distinct concavities seen in
lower
borders of C2 and C3
Concavity is developing in lower
border of C4
C3 and C4 are rectangular in
shape
2.
3.
4.25-65% of pubertal growth
remains
26.
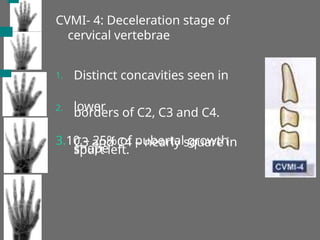
CVMI- 4: Decelerationstage of
cervical vertebrae
1. Distinct concavities seen in
lower
borders of C2, C3 and C4.
C3 and C4 – nearly square in
shape
2.
3.10 – 25% of pubertal growth
spurt left.
27.
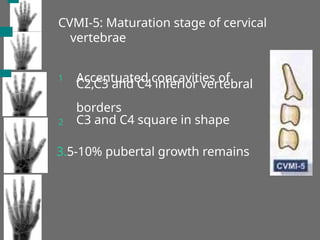
CVMI-5: Maturation stageof cervical
vertebrae
1 Accentuated concavities of
C2,C3 and C4 inferior vertebral
borders
C3 and C4 square in shape
2
3.5-10% pubertal growth remains
28.
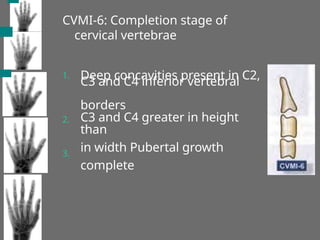
CVMI-6: Completion stageof
cervical vertebrae
1. Deep concavities present in C2,
C3 and C4 inferior vertebral
borders
C3 and C4 greater in height
than
in width Pubertal growth
complete
2.
3.
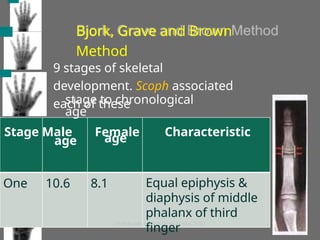
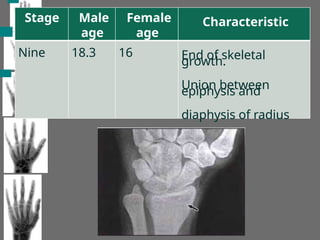
Bjork, Grave andBrown
Method
One 10.6 8.1
9 stages of skeletal
development. Scoph associated
each of these
stage to chronological
age
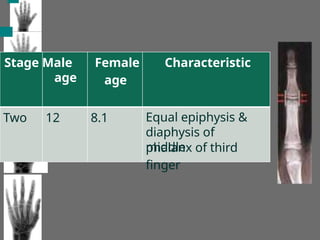
Stage Male Female
age
Characteristic
age
Equal epiphysis &
diaphysis of middle
phalanx of third
finger
bone
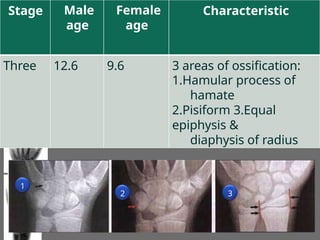
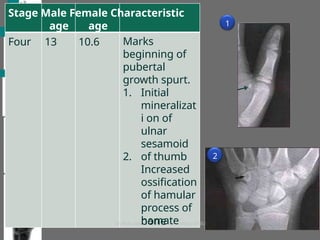
Stage Male FemaleCharacteristic
Four
age
13
age
10.6 Marks
beginning of
pubertal
growth spurt.
1. Initial
mineralizat
i on of
ulnar
sesamoid
of thumb
Increased
ossification
of hamular
process of
hamate
2. 2
1
34.
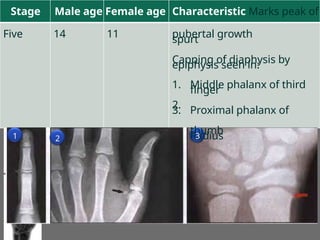
Stage Male ageFemale age Characteristic Marks peak of
pubertal growth
spurt
Capping of diaphysis by
epiphysis seen in:
Five 14 11
1.
2.
3.
Middle phalanx of third
finger
Proximal phalanx of
thumb
Radius
1 2 3
35.
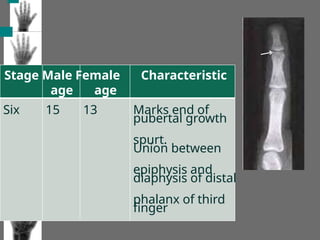
Stage Male FemaleCharacteristic
age age
Six 15 13 Marks end of
pubertal growth
spurt.
Union between
epiphysis and
diaphysis of distal
phalanx of third
finger
36.
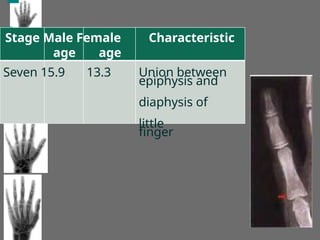
Stage Male FemaleCharacteristic
age age
Seven 15.9 13.3 Union between
epiphysis and
diaphysis of
little
finger
37.
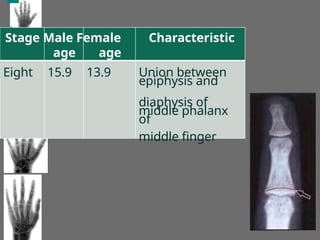
Stage Male FemaleCharacteristic
age age
Eight 15.9 13.9 Union between
epiphysis and
diaphysis of
middle phalanx
of
middle finger
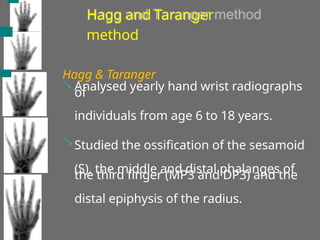
Hagg and Taranger
method
Hagg& Taranger
Analysed yearly hand wrist radiographs
of
individuals from age 6 to 18 years.
Studied the ossification of the sesamoid
(S), the middle and distal phalanges of
the third finger (MP3 and DP3) and the
distal epiphysis of the radius.
40.
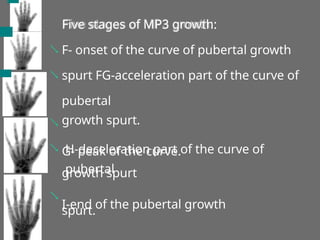
Five stages ofMP3 growth:
F- onset of the curve of pubertal growth
spurt FG-acceleration part of the curve of
pubertal
growth spurt.
G- peak of the curve.
H-deceleration part of the curve of
pubertal
growth spurt
I-end of the pubertal growth
spurt.
MP3-F Stage
Start ofthe curve of pubertal
growth
spurt
Epiphysis is as wide as
metaphysis
End of epiphysis are tapered
and
rounded.
Radiolucent gap is wide
between
epiphysis & diaphysis.
80-100% of pubertal growth remains.
Initiation stage of cervical vertebrae
C2,C3 and C4 inferior vertebral
body borders are flat.
Superior vertebral borders are tapered from
posterior to anterior [wedge shape]
CVMI-1
43.
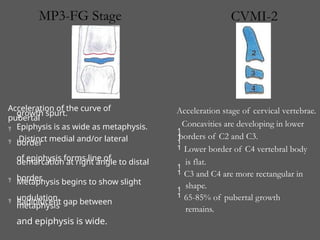
Acceleration of thecurve of
pubertal
growth spurt.
Epiphysis is as wide as metaphysis.
Distinct medial and/or lateral
border
of epiphysis forms line of
demarcation at right angle to distal
border.
Metaphysis begins to show slight
undulation.
Radiolucent gap between
metaphysis
and epiphysis is wide.
Lower border of C4 vertebral body
is flat.
C3 and C4 are more rectangular in
shape.
65-85% of pubertal growth
remains.
Acceleration stage of cervical vertebrae.
Concavities are developing in lower
borders of C2 and C3.
MP3-FG Stage CVMI-2
44.
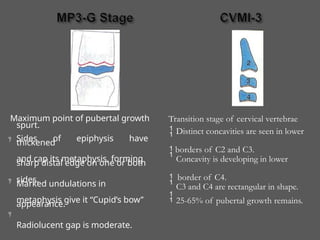
Maximum point ofpubertal growth
spurt.
Sides of epiphysis have
thickened
and cap its metaphysis, forming
sharp distal edge on one or both
sides.
Marked undulations in
metaphysis give it “Cupid’s bow’’
appearance.
Radiolucent gap is moderate.
Transition stage of cervical vertebrae
Distinct concavities are seen in lower
borders of C2 and C3.
Concavity is developing in lower
border of C4.
C3 and C4 are rectangular in shape.
25-65% of pubertal growth remains.
45.
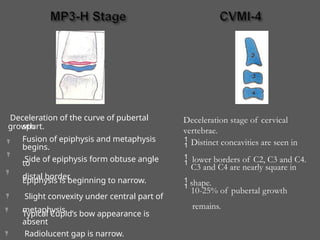
Deceleration of thecurve of pubertal
growth
spurt.
Fusion of epiphysis and metaphysis
begins.
Side of epiphysis form obtuse angle
to
distal border.
Epiphysis is beginning to narrow.
Slight convexity under central part of
metaphysis.
Typical Cupid’s bow appearance is
absent
Radiolucent gap is narrow.
Deceleration stage of cervical
vertebrae.
Distinct concavities are seen in
lower borders of C2, C3 and C4.
C3 and C4 are nearly square in
shape.
10-25% of pubertal growth
remains.
46.
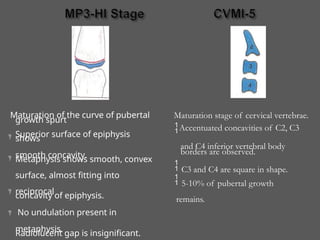
Maturation of thecurve of pubertal
growth spurt
Superior surface of epiphysis
shows
smooth concavity.
Metaphysis shows smooth, convex
surface, almost fitting into
reciprocal
concavity of epiphysis.
No undulation present in
metaphysis.
Radiolucent gap is insignificant.
Maturation stage of cervical vertebrae.
Accentuated concavities of C2, C3
and C4 inferior vertebral body
borders are observed.
C3 and C4 are square in shape.
5-10% of pubertal growth
remains.
47.
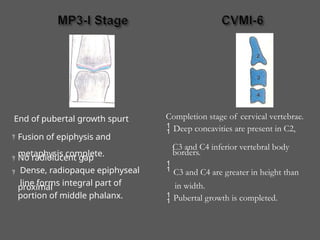
End of pubertalgrowth spurt
Fusion of epiphysis and
metaphysis complete.
No radiolucent gap
Dense, radiopaque epiphyseal
line forms integral part of
proximal
portion of middle phalanx.
in width.
Pubertal growth is completed.
Completion stage of cervical vertebrae.
Deep concavities are present in C2,
C3 and C4 inferior vertebral body
borders.
C3 and C4 are greater in height than
48.
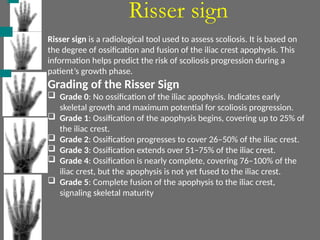
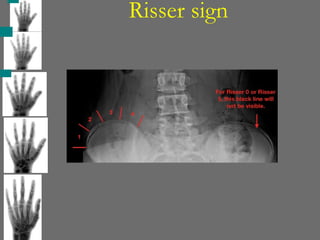
Risser sign
Risser signis a radiological tool used to assess scoliosis. It is based on
the degree of ossification and fusion of the iliac crest apophysis. This
information helps predict the risk of scoliosis progression during a
patient’s growth phase.
Grading of the Risser Sign
Grade 0: No ossification of the iliac apophysis. Indicates early
skeletal growth and maximum potential for scoliosis progression.
Grade 1: Ossification of the apophysis begins, covering up to 25% of
the iliac crest.
Grade 2: Ossification progresses to cover 26–50% of the iliac crest.
Grade 3: Ossification extends over 51–75% of the iliac crest.
Grade 4: Ossification is nearly complete, covering 76–100% of the
iliac crest, but the apophysis is not yet fused to the iliac crest.
Grade 5: Complete fusion of the apophysis to the iliac crest,
signaling skeletal maturity
Risser sign
Clinical Importance:
TheRisser sign is a key component in scoliosis
management, as it helps predict growth potential and the
risk of curve progression.
Low Risser grades (0–2): Indicate active growth phases
with a higher risk of scoliosis progression.
High Risser grades (3–5): Suggest reduced growth
potential and a lower risk of scoliosis worsening.
Limitations:
Differences in Risser grading systems exist between the
U.S. and Europe, with slight variations in interpretation.
Other methods like the Tanner staging and hand-wrist
radiographs may also be used for growth assessment in
conjunction with the Risser sign.
![MP3-F Stage
Start of the curve of pubertal
growth
spurt
Epiphysis is as wide as
metaphysis
End of epiphysis are tapered
and
rounded.
Radiolucent gap is wide
between
epiphysis & diaphysis.
80-100% of pubertal growth remains.
Initiation stage of cervical vertebrae
C2,C3 and C4 inferior vertebral
body borders are flat.
Superior vertebral borders are tapered from
posterior to anterior [wedge shape]
CVMI-1](https://image.slidesharecdn.com/skeletalmaturityindicatorsgavicopy-250627163500-51d51a69/85/SKELETALMATURITYINDICATORS-GAVI-copy-pptx-42-320.jpg)