INTRODUCTION
An understanding ofgrowth events is of primary
importance in the practice of clinical orthodontics.
Chronological age, appearance of secondary sexual
characters, growth charts, dental development and
skeletal maturation are often used for growth prediction
in clinical orthodontic practice.
Due to individual variations in timing, duration and
velocity of growth, skeletal age assessment is essential
in formulating viable orthodontic treatment plans.
Although a number of skeletal maturity indicators have
been described, the hand –wrist radiograph is the most
accepted one.
3.
MATURITY INDICATORS
The keyto successful treatment is to start at right age.
There are a number of maturity indicators.
Neural age
Mental age
Physiologic age
Chronological age chronological age is defined as the
time period from the birth to till date.
Morphologic age is based on the height stands in
relation to others. Height is useful as a maturity
indicator from late infancy to early adulthood.
4.
Sexual age Sexualage refers to development
of secondary sexual characteristics. This type
of indicator is useful only for adolescent
growth.
Dental age Dental age has been based on two
different methods of assessment.
1. Tooth eruption age.
2. Tooth mineralization stage.
Age determination using growth chart.
Skeletal/anatomical/radiological age
5.
Growth Spurt
A spurtis defined as growth acceleration
up to a maximum where the annual
increment of growth exceeded the
previous one by at least 0.7mm
-Erkstrom.
6.
Just one yearbefore birth
One year after birth.
Mixed dentition growth spurt.
boys 8-11 years
girls 7-9 years
Pre pubertal growth spurt
boys 14- 16 years
girls 11-13 years
7.
Developmental statusof the child judged by :
i. peak height velocity
ii. menarche in case of girls
iii. voice change in boys
iv. dental development
v. skeletal ossification
8.
REQUIREMENTS OF ANIDEAL
MATURITY INDICATOR
Ideal requirements for maturity indicators include
Should be safe
Non-invasive
Requires minimum radiation
Should be accurate
Stages of maturity should be well defined
Cost effective
Minimum armamentarium and personnel requirement
Method should be simple to conduct.
Should be valid across age and time groups
9.
CLINICAL IMPORTANCE
Detecting potentialvector for facial
development.
Determining amount of significant facial
cranial growth potential left.
To evaluate rate of growth.
To decide the onset of treatment timing.
10.
To decide typeof effective treatment
a) Orthopedic
Removable
Fixed
b)Orthodontic
c)Orthognathic surgical procedure
d)Combination of the above
To evaluate treatment prognosis.
To understand the role of genetics and
environment on skeletal maturation pattern.
11.
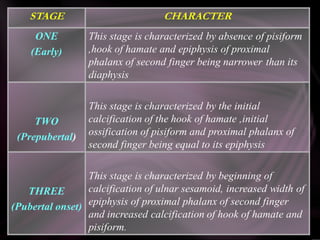
LATE AND EARLYDEVELOPMENT
Sixtypes of skeletal development has been
recognized.
GROUP CHARACTER
1st group
2nd group
average children
Children who are tall in childhood
only because they have matured faster
than average. They will not be
particularly tall adults
12.
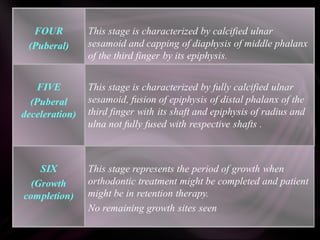
3rd group
4th group
5thgroup
6th group
children who not only mature early but who
are generally tall. The children are taller than
average from early childhood and will be tall
adults.
Children who are small because they mature
late.
Children who are both late in developing and
genetically short in stature.
Indefinite group who mature much early or
much late than usual .
13.
ANATOMIC REGIONS OFASSESSMENT
The anatomic regions suitable for skeletal
maturational assessment should have ideally
Region should be small to limit radiation exposure
and expense.
Should have many ossification centers which ossify at
separate time and which can be standardized.
Region should be easily accessible
14.
Regions normally usedfor age assessment
Head and neck:
• Skull
• Cervical vertebrate
Upper limb:
• Shoulder joint –scapula
• Elbow
• Hand wrist and fingers
Lower limb:
• Femur and humerus
• Hip joint
• Knee
• Ankle
• Foot-tarsal
• Metatarsals
• Phalanges
15.
Skeletal maturity indicators
Hand and wrist radiographs,
Cervical vertebrae
Mid palatal suture
Corpus index
Tooth mineralization
Orthodontic treatment progressesmore quickly
during growth spurts. Generally children
experience a pattern of fast growth,
followed by a slow growth in late childhood
and then accelerated and peak growth in
adolescence. Because children begin this
sequence of growth at different ages,
chronological age is a poor indicator of a
child’s development. Hand-wrist radiograph
is a useful tool for identifying a child’s
skeletal development.
18.
The hand wristregion is made of numerous
small bones. These bones show a predictable
and scheduled pattern of appearance,
ossification and union from birth to
maturity.Hence,this region is one of the most
suited to study growth.
19.
IMPORTANCE OF HANDWRIST RADIOGRAPH
IN ORTHODONTICS
Carpal bone, phalanges, metacarpals provide a clue to
bone growth as a whole.
Inspection of carpal radiographs to assess the growth
by evaluating the following:
– Shape of the carpal bone
– Degree of ossification of the skeleton.
– Time and order of appearance
DISADVANTAGE
– The site of radiation is a bit away from the site of
clinical examination i.e. the oral cavity
20.
TECHNIQUE
Patient is seatedwith the forearm on the
table on a line parallel with his
shoulder
Loaded cassette is placed on the table,
below the hand with its long axis
parallel to the hand.
The central ray is directed
perpendicular to a line passing between
the hands and if only one hand is to be
radiographed, the central ray should be
directed at centre of the carpals.
21.
Indications of HandWrist Radiographs
Patients exhibit major discrepancy between dental and
chronological age.
Determination of skeletal age prior to treatment of skeletal
malocclusion such as skeletal class II or Class III.
Assess skeletal age in patients whose growth is affected by
infections, neoplastic or traumatic conditions.
Serial assessment helps not only in assessing growth of an
individual but also helps predicts future skeletal maturation
rate and status.
22.
To assess pubertalgrowth spurt.
Valuable aid in research aimed at studying the role of
heredity, environment, nutrition etc, on skeletal
maturation pattern
.
Prior to rapid maxillary expansion
In patients with skeletal malocclusion needing
orthognathic surgery, if undertaken between 16-20
years so as to assess the growth status.
23.
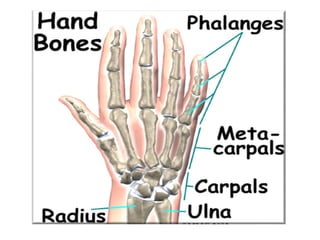
ANATOMY OF HANDWRIST
The hand wrist is made of the following four groups of
bones:
Distal end of long bones of forearm
Carpals
Metacarpals
Phalanges
25.
Distal end oflong bones
The distal end of radius and ulna, which are the long
bones of the forearm, were initially used for the
purpose of skeletal age determination.
In anatomical position, with the palm facing the front,
the ulna is on the medial aspect while radius is on the
distal aspect.
The radius and ulna gives rise to a distal projection on
their respective sides.
26.
The Carpels
They consistof 8 small, irregularly shaped bones arranged in two
rows- a proximal row and a distal row.
Bones of proximal row Bones of distal row
• Scaphoid Trapezium
• Lunate Trapezoid
• Triquetral Capitate
• Pisiform Hamate
Each of these eight carpal bone ossifies from one primary
centre ,which appears in a predictable manner.
27.
The Metacarpals
• 5miniature long bones forming the skeletal framework of the
palm of the human hand.
• All the metatarsals ossify from one primary centre located in
their shafts and a secondary centre on their distal end (except in
the first metacarpal where it appears at the proximal end.
The Sesamoid
• The sesamoid bone is a small nodular bone most often present
embedded in the tendons in the region of the thumb.
28.
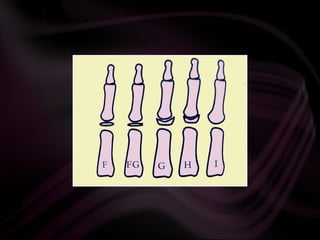
The Phalanges
Smallbones that form the finger.
Three phalanges in each finger. Thumb has only two
phalanges.
The three phalanges are:
– Proximal
– Middle (absent in the thumb)
– Distal phalanges
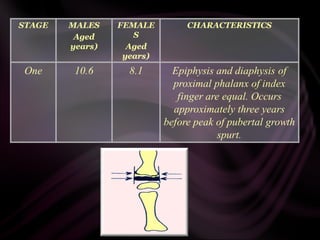
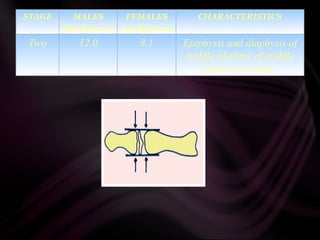
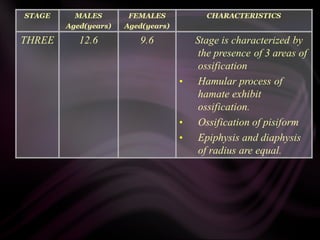
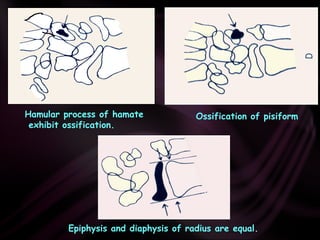
Ossification of phalanges:
Occurs in three stages
29.
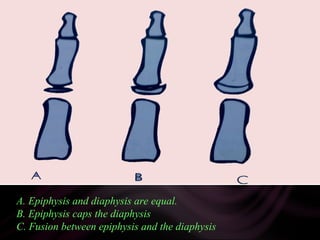
A.
A. Epiphysis anddiaphysis are equal.
B. Epiphysis caps the diaphysis
C. Fusion between epiphysis and the diaphysis
30.
A number ofmethods have been described to
assess the skeletal maturity using hand-wrist
radiographs. The following are the most
commonly used methods:
Atlas method by Greulich and Pyle
Bjork, Grave and Brown method
Fishman’s skeletal maturity indicator
Hagg and Taranger method.
32.
Greulich and Pylepublished an atlas containing
ideal skeletal age picture of the hand wrist for
different chronological age and for each sex.
The atlas is composed of plates of “typical” hand-
wrist radiographs at six-month intervals of
chronological age.
Each bone of the subject's hand-wrist is compared
with the corresponding bones in the atlas and is
assigned an age in months.
All ages are averaged yielding the “mean age” of the
individual.
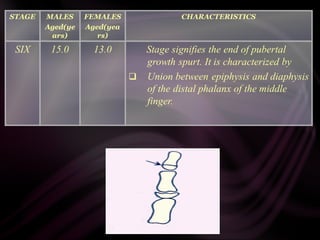
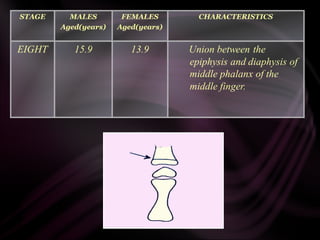
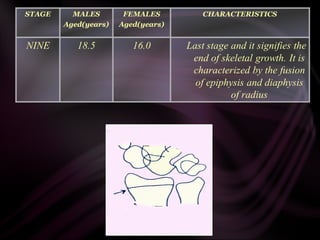
They have dividedthe skeletal development
into nine stages.
Each of this stage represents a level of skeletal
maturity.
Schoph in 1978 associated each of this stage
with a particular chronological age.
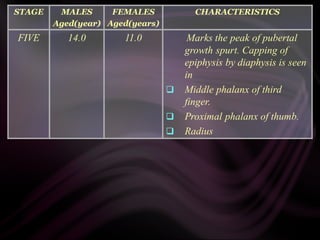
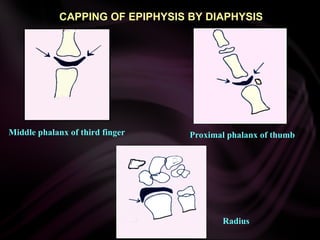
CAPPING OF EPIPHYSISBY DIAPHYSIS
Middle phalanx of third finger Proximal phalanx of thumb
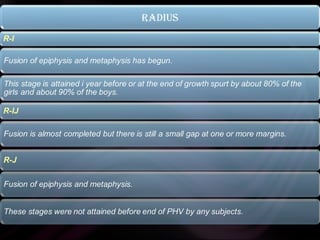
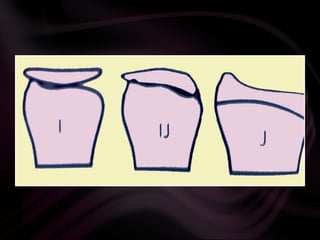
Radius
48.
Julian singer in1980 proposed a system of age
assessment which was far quicker and had
some degree of reliability to help determine
the maturational status of a patient. Six stages
of hand-wrist development are explained.
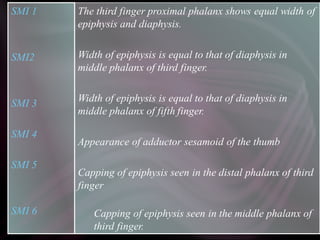
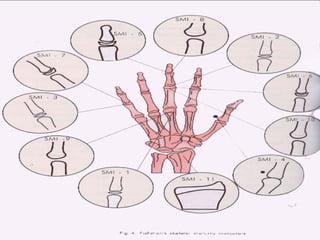
A system ofevaluation skeletal maturation was proposed by Leonard S
Fishman in 1982. Fishman made use of 4 anatomical sites located on
The thumb
The third finger
The fifth finger
The radius
Eleven discrete adolescent skeletal maturity indicators (SMI) was
proposed which covered the entire period of adolescent development.
The Fishman system of interpretation uses 4 stages of bone
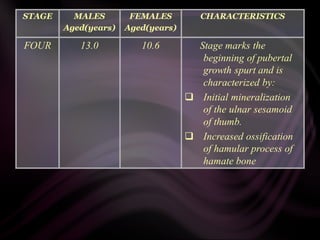
maturation which include:
Epiphysis is equal in width to diaphysis
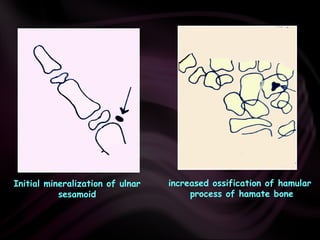
Appearance of adductor sesamoid of thumb
Capping of epiphysis.
Fusion of epiphysis.
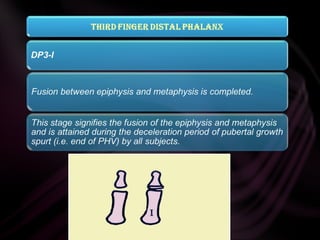
54.
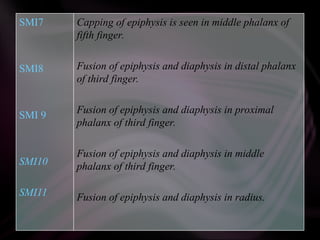
SMI7
SMI8
SMI 9
SMI10
SMI11
Capping ofepiphysis is seen in middle phalanx of
fifth finger.
Fusion of epiphysis and diaphysis in distal phalanx
of third finger.
Fusion of epiphysis and diaphysis in proximal
phalanx of third finger.
Fusion of epiphysis and diaphysis in middle
phalanx of third finger.
Fusion of epiphysis and diaphysis in radius.
57.
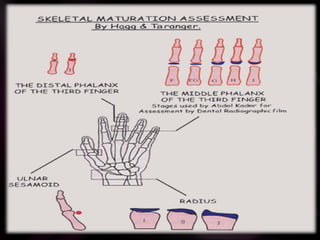
Skeletal development inthe hand and wrist is analyzed
from annual radiographs ,taken from age 6- 18 yrs and
by the assessment of the ulnar sesamoid of the
metacarpophalangeal joint of the first finger (S) and
certain specified stages of three epiphyseal bones.
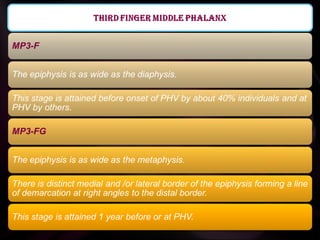
Middle phalange of third finger.
Distal phalange of third finger.
Distal epiphysis of radius.
Kansal and Rajagopal modified the MP3 indicators
further and compared it to the cervical vertebrate
maturation indices as described by Hassel and Farman.
58.
SESAMOID
Sesamoid is usuallyattained during the
acceleration period of pubertal growth spurt.
( onset of peak height velocity)
• The firstseven vertebrae in the spinal column constitute
the cervical spine. The first two, the atlas and the
axis are quite unique, the third through the seventh
have great similarity. Maturational changes can be
observed from birth to full maturity.
• Vertebral growth takes place from the cartilagenous layer
on the superior and inferior surface of each
vertebrae. Secondary ossification nuclei on the tips of
the bifid spinous processes and transverses appear during
puberty.
• After completion of endochondral ossification, growth
of the vertebral body takes place by periosteal apposition.
It appears to take place only at the front and
sides.Lamparski studied changes in size and shape of
cervical vertebrae .
68.
Hassel and Farmandeveloped a system of skeletal maturation
determination using the cervical vertebrate. The shape of the
cervical vertebrate was seen to differ at each stage of skeletal
development.
• Shape of vertebral from wedge shaped rectangular
square
• They also become taller as skeletal maturity progresses
• Inferior vertebral bodies--- flat (immature)
Concave (mature)
• On maturation curvature of inferior vertebral borders were seen to
appear sequentially from C2 to C3 to C4 as skeleton matured.
• Hassel and Farman put forward six stages of vertebral
development.
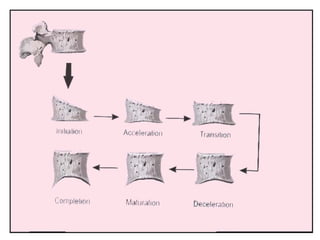
70.
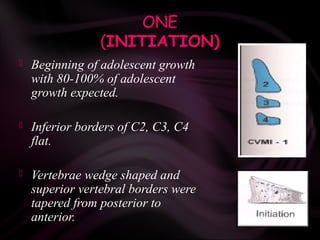
ONE
(INITIATION)
Beginning ofadolescent growth
with 80-100% of adolescent
growth expected.
Inferior borders of C2, C3, C4
flat.
Vertebrae wedge shaped and
superior vertebral borders were
tapered from posterior to
anterior.
71.
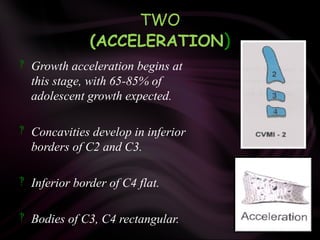
TWO
(ACCELERATION)
Growth accelerationbegins at
this stage, with 65-85% of
adolescent growth expected.
Concavities develop in inferior
borders of C2 and C3.
Inferior border of C4 flat.
Bodies of C3, C4 rectangular.
72.
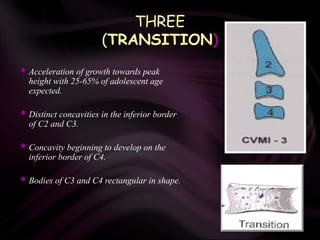
THREE
(TRANSITION)
Acceleration ofgrowth towards peak
height with 25-65% of adolescent age
expected.
Distinct concavities in the inferior border
of C2 and C3.
Concavity beginning to develop on the
inferior border of C4.
Bodies of C3 and C4 rectangular in shape.
73.
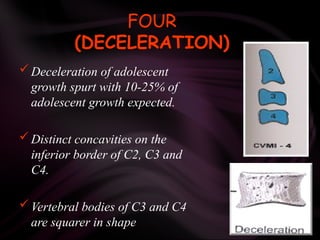
FOUR
(DECELERATION)
Deceleration ofadolescent
growth spurt with 10-25% of
adolescent growth expected.
Distinct concavities on the
inferior border of C2, C3 and
C4.
Vertebral bodies of C3 and C4
are squarer in shape
74.
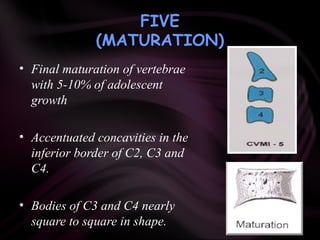
FIVE
(MATURATION)
• Final maturationof vertebrae
with 5-10% of adolescent
growth
• Accentuated concavities in the
inferior border of C2, C3 and
C4.
• Bodies of C3 and C4 nearly
square to square in shape.
75.
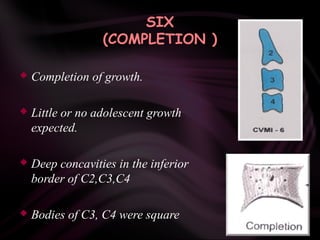
SIX
(COMPLETION )
Completionof growth.
Little or no adolescent growth
expected.
Deep concavities in the inferior
border of C2,C3,C4
Bodies of C3, C4 were square
76.
TOOTH MINERALIZATION ASAN
INDICATOR OF SKELETAL MATURITY
The calcification patterns and stages of mineralization of teeth is
believed to have a close relationship to the skeletal maturation of
an individual.
Seymour Chertkow has described a method of determining skeletal
maturity by based on the mineralization of the lower canine.
Demirjain, Goldstein and Tanner have also described a similar
method.
77.
Demirjian et al.,in 1973 divided tooth
mineralization into nine stages
Dental age determination according to the
stage of mineralization
78.
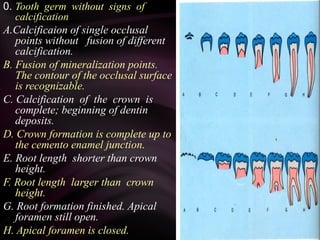
0. Tooth germwithout signs of
calcification
A.Calcificaion of single occlusal
points without fusion of different
calcification.
B. Fusion of mineralization points.
The contour of the occlusal surface
is recognizable.
C. Calcification of the crown is
complete; beginning of dentin
deposits.
D. Crown formation is complete up to
the cemento enamel junction.
E. Root length shorter than crown
height.
F. Root length larger than crown
height.
G. Root formation finished. Apical
foramen still open.
H. Apical foramen is closed.
79.
Completion of rootformation of
mandibular canine, prior to apical closure
80.
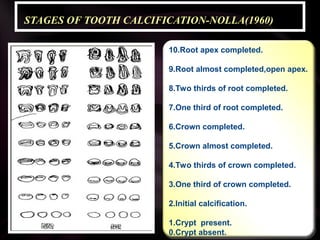
STAGES OF TOOTHCALCIFICATION-NOLLA(1960)
10.Root apex completed.
9.Root almost completed,open apex.
8.Two thirds of root completed.
7.One third of root completed.
6.Crown completed.
5.Crown almost completed.
4.Two thirds of crown completed.
3.One third of crown completed.
2.Initial calcification.
1.Crypt present.
0.Crypt absent.
81.
CONCLUSION
Chronological age isnot a valid predictor of skeletal growth
velocity or skeletal maturity. The validity of skeletal maturity
assessment using the hand-wrist radiograph in relation to
overall skeletal growth velocity (standing height) has been well
established and has been validated for several racial groups.
Correlation of skeletal age determined with the Greulich and
Pyle atlas and the Tanner et al analysis is good. However,
interpretation of the accuracy of skeletal age for predicting
growth may be improved if other parameters -morphologic,
biological, or genetic indicators, in addition to hand-wrist
radiographic evaluation are used.