Why do weneed to know about shock??
● SHOCK IS MOST COMMON AND MOST IMPORTANT
CAUSE OF DEATH IN SURGICAL PATIENTS.
4.
DEFINITION
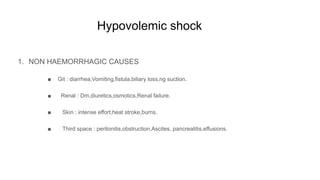
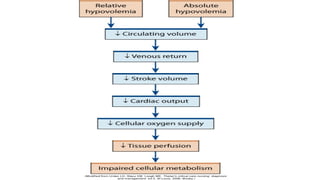
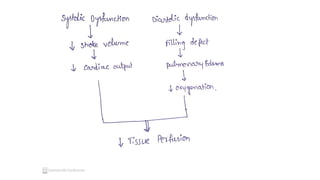
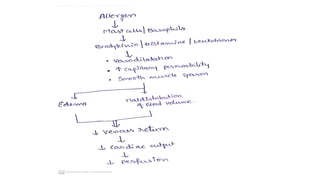
Shock is asystemic state of low tissue
perfusion that is inadequate for normal
cellular respiration.
5.
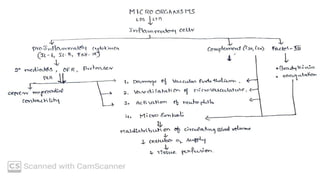
PHYSIOLOGY
● Cell isthe structural and functional unit of the body.
● For the functioning of cell - oxygen and glucose is required.
● Perfusion depends on - pump,vessels,Volume.
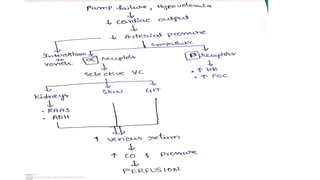
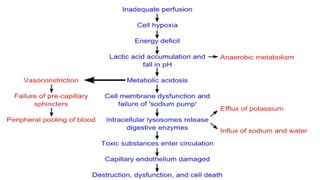
Cellular : metabolicacidosis due to anaerobic
metabolism.
Cell lysis due to auto Digestive enzymes by
lysosomes.
Microvascular : damage of endothelium due to OFR.
Systemic :
● CVS : baroreceptors - catecholamines.
● RS : Compensatory Respiratory alkalosis to MA.
● Renal : RAAS - sodium and water reabsorption.
● ENDOCRINE : ADH -Na and water reabsorpbed
CORTISOL.
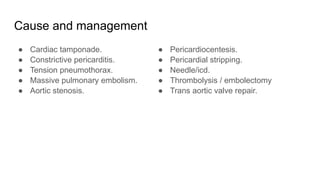
2. HAEMORRHAGIC CAUSES
●Wounds
● Hemetemesis, melena, hemoptysis, epistaxis .
● Hemothorax,hemoperitoneum.
Fluid loss is absolute or relative( third space loss).
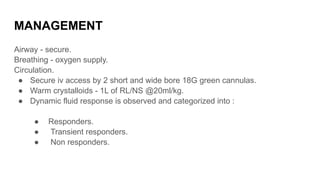
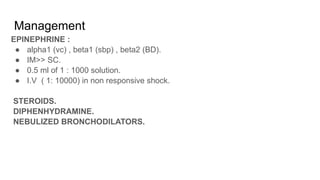
MANAGEMENT
Airway - secure.
Breathing- oxygen supply.
Circulation.
● Secure iv access by 2 short and wide bore 18G green cannulas.
● Warm crystalloids - 1L of RL/NS @20ml/kg.
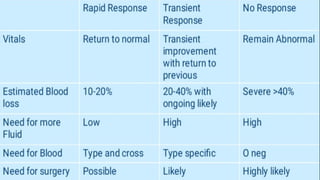
● Dynamic fluid response is observed and categorized into :
● Responders.
● Transient responders.
● Non responders.
20.
BLOOD
● Crash 2trial (BP<90 mmhg ; PR >110/ min) - 1gm tranexamic acid in 10 mins
followed by 1gm in 8 hrs.
● Monitor for Acute traumatic coagulopathy -avoid crystalloids due to risk of
dilutional coagulopathy - so give blood.
● Blood group O negative for reproductive females and O positive for males and
post reproductive females.
● Balanced resuscitation ( 1:1:1 prbc : plt : plasma).
● Permissible hypotension(70-90) maintained to prevent rebleeding and hypoxia.
● Massive transfusion protocol ( >10u in 24hrs or >4 units in a hour ).
● Replacement of clotting factors if required.
21.
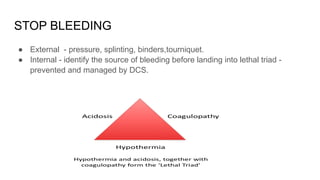
STOP BLEEDING
● External- pressure, splinting, binders,tourniquet.
● Internal - identify the source of bleeding before landing into lethal triad -
prevented and managed by DCS.
Poor prognostic factors
●Advanced age.
● Immunosuppression.
● Resistant organism.
● Level of IL-6.
● Need for inotropes >24 hrs.
● Mods despite Treatment.
43.
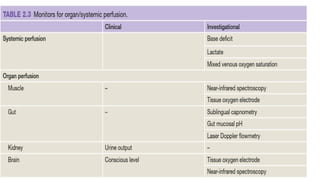
Markers of sepsis
●Procalcitonin
a. Value of >2.0 IU/ml suggests severe sepsis.
b. Best marker of sepsis.
c. Best guide of antibiotic treatment.
● CRP. - highly sensitive.
45.
● qSOFA Score: quick sequential organ failure assessment score.
A. Respiratory rate - > 22 / min.
B. Confused mental status.
C. BP - < 100 mmhg.
A score of >2 suggests poor outcome.
46.
SURVIVING SEPSIS GUIDELINES: Parameters to be met in first 6 hrs.
● CVP - 8 to 12.
● MAP - >/= 65 mmhg.
● URINE OUTPUT - >/= O.5 ml/kg/hr.
● MVOS - 65%.
● SVC Oxygen saturation - 70%.
47.
Prevention
● Early recognition.
●Prompt treatment of infection.
● Meticulous surgical technique.
● Pre-op antibiotics.
● Aseptic techniques.
● Sterilization of equipment.
● Hypothyroidism -decrease cardiac output - levothyroxine.
● Hyperthyroidism - reversible cardiomyopathy - methimazole,ptu.
● Acute adrenal insufficiency - steroids.
A. Not tapered.
B. Surgery for pt on corticosteroid.
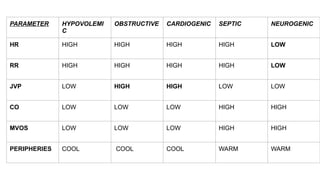
PARAMETER HYPOVOLEMI
C
OBSTRUCTIVE CARDIOGENICSEPTIC NEUROGENIC
HR HIGH HIGH HIGH HIGH LOW
RR HIGH HIGH HIGH HIGH LOW
JVP LOW HIGH HIGH LOW LOW
CO LOW LOW LOW HIGH HIGH
MVOS LOW LOW LOW HIGH HIGH
PERIPHERIES COOL COOL COOL WARM WARM
67.
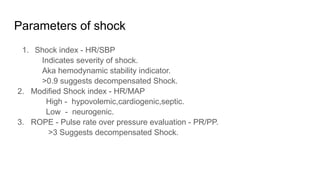
Parameters of shock
1.Shock index - HR/SBP
Indicates severity of shock.
Aka hemodynamic stability indicator.
>0.9 suggests decompensated Shock.
2. Modified Shock index - HR/MAP
High - hypovolemic,cardiogenic,septic.
Low - neurogenic.
3. ROPE - Pulse rate over pressure evaluation - PR/PP.
>3 Suggests decompensated Shock.
70.
URINE OUTPUT
● Bestclinical indicator of tissue perfusion.
● Best indicator of fluid resuscitation.
● Normal values :
Adults - >0.5 ml/kg/hr.
Children - >1 ml/kg/hr.
71.
CENTRAL VENOUS PRESSURE
●Normal value - 0 to 8.
● Measured by cvc and a manometer or transducer.
● fluid bolus (250 to 500 mL) is infused rapidly over 5–10 minutes and cvp
measured - increase of 2 to 5 cmh2o and becomes normal in 10 to 20 mins.
A. No change - further resuscitation is required.
B. Increased - implies cardiac insufficiency or overload.
● Best method to calculate amount of fluid to be given.
72.
Base deficit
● Amountof base required to titrate a litre of whole arterial blood to a ph of 7.4.
● Normal value is -2 to +2 meq/l.
● Value below -2 suggests metabolic acidosis.
● Value above +2 suggests metabolic alkalosis.
73.
Serum Lactate
● Bestlab value to monitor tissue perfusion.
● Normal lactate value is 0.5 to 1 mmol/l.
● Value of <2 ~ good resuscitation.
● Value of >5 ~ bad resuscitation.
● Best to look for git and muscle perfusion.
74.
Mixed venous oxygensaturation
● The percentage saturation of oxygen returning to the heart from the body is a
measure of the oxygen delivery and extraction by the tissues.
● Measured in blood drawn from Central lines in right atrium or SVC.
● Normal range - 50 to 70 %.
● Low Mvos - hypovolemic and cardiogenic shocks.
● High Mvos - septic and neurogenic.
75.
END POINTS OFRESUSCITATION
● State of normal vital signs and continued underper fusion is termed -occult
hypoperfusion.
● Time spent in this state proportional to morbidity and mortality.
● Base deficit,lactate, Mvos are best measures to end resuscitation rather than
relying on vital signs.



















































![SUJATsdsdsdsdsdsdsdsdsdfsaf HA[thesis ppt] (1).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/sujathathesisppt1-250813130511-b7c36e11-thumbnail.jpg?width=640&height=640&fit=bounds)

























