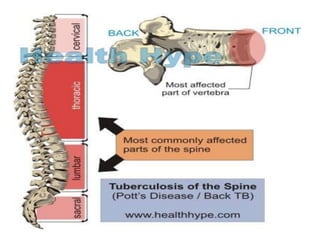
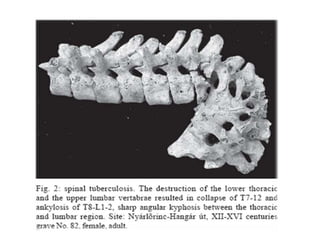
Tuberculosis can infect the vertebrae and bones, usually spreading from the lungs via blood. It causes osteomyelitis and arthritis, often affecting the lower thoracic and upper lumbar vertebrae. Symptoms include localized back pain, fever, weight loss, and sometimes neurological signs. Diagnosis involves tests showing elevated ESR, positive Mantoux test, and MRI identifying bone changes. Treatment involves antibiotics and sometimes surgery to correct spinal instability or decompress the spinal cord.