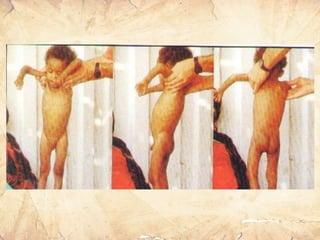
Malnutrition, especially protein-energy malnutrition (PEM), is a leading cause of death in children under 5 years old globally and in India. The document discusses the etiology, classifications, clinical features, complications and management of PEM. PEM results from a combination of low food intake and frequent infections. It manifests as marasmus (wasting without edema) or kwashiorkor (wasting with edema). Treatment involves medical management of complications, nutritional rehabilitation with formula diets or food, and management of underlying causes like poverty and feeding practices.