Download as PDF, PPTX

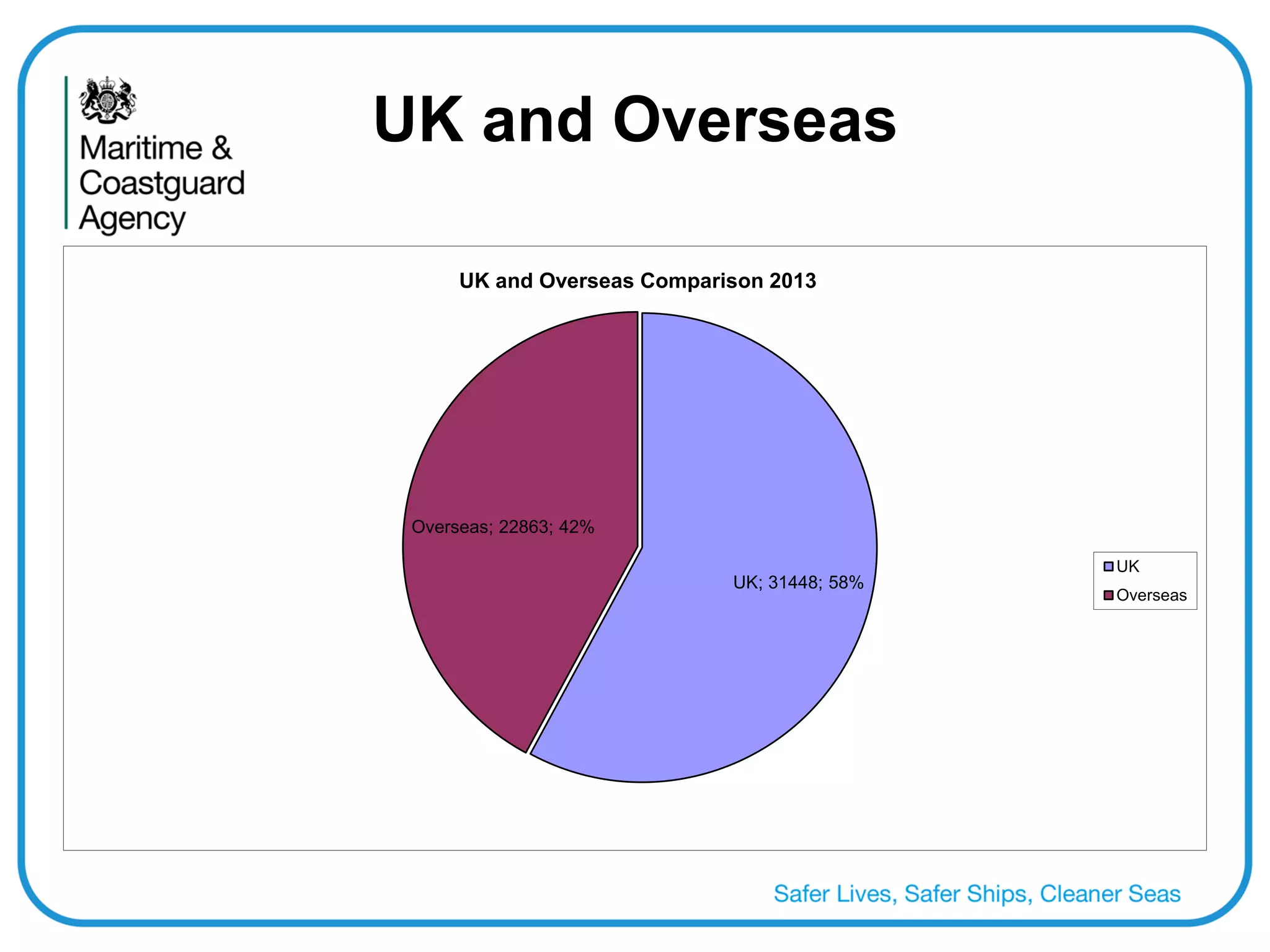


The document discusses the UK system for approving doctors to conduct seafarer medical examinations and potential international collaboration on mutual recognition. It notes there are 225 approved doctors in the UK and overseas, who conducted over 54,000 examinations in 2013. The UK provides support to doctors through medical standards, training, and oversight. International meetings have discussed aligning medical standards between countries like Norway, Germany, the Netherlands and the UK. While progress has been made in understanding each other's systems, further work is still needed before mutual recognition of approved doctors across countries can be achieved.






![Session 3 6 - dr. n.nikolić [reparert]](https://cdn.slidesharecdn.com/ss_thumbnails/session3-6-dr-140905042744-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




































![D ay 2 3_imhaquality for ncmm sally bell[1]](https://cdn.slidesharecdn.com/ss_thumbnails/day23imhaqualityforncmmsallybell1-120502022843-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![D ay 2 3_imhaquality for ncmm sally bell[1]](https://cdn.slidesharecdn.com/ss_thumbnails/day23imhaqualityforncmmsallybell1-120502024315-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Carter seahealth 4 12 tim [1]](https://cdn.slidesharecdn.com/ss_thumbnails/carterseahealth412tim1-120502022829-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Carter seahealth 4 12 tim [1]](https://cdn.slidesharecdn.com/ss_thumbnails/carterseahealth412tim1-120502023845-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Day 2 1 carter seahealth 4 12[1]](https://cdn.slidesharecdn.com/ss_thumbnails/day21carterseahealth4121-120502024059-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Day 2 1 carter seahealth 4 12[1]](https://cdn.slidesharecdn.com/ss_thumbnails/day21carterseahealth4121-120502022839-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)












![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)









