Sepsis is a life-threatening organ dysfunction caused by a dysregulated immune response to infection, which can rapidly lead to tissue damage, organ failure, and death if not treated promptly. Common causes include bacterial infections like pneumonia and UTIs, and symptoms include fever, altered mental status, and low blood pressure. Diagnosis involves assessing for signs of infection and organ dysfunction using tools like SOFA and lactate levels, and treatment focuses on early antibiotic administration, fluid resuscitation, and vasopressor support if needed to stabilize the patient.
What is sepsis?
• Sepsis is a life-threatening organ dysfunction caused by a
dysregulated host response to infection.
• Sepsis is the body’s extreme response to an infection. It is a life-
threatening medical emergency.
• Sepsis happens when an infection you already have triggers a chain
reaction throughout your body. Most cases of sepsis start before a
patient goes to the hospital.
• Without timely treatment, sepsis can rapidly lead to tissue damage,
organ failure, and death.
3.
Epidemiology
• A recentscientific publication estimated that in 2017 there were 48.9
million cases and 11 million sepsis-related deaths worldwide, which
accounted for almost 20% of all global deaths.
• In 2017, almost half of all global sepsis cases occurred among
children, with an estimated 20 million cases and 2.9 million global
deaths in children under 5 years of age.
• approximately 85% of sepsis cases and sepsis-related deaths
worldwide occurred in low- and middle-income countries.
• Health care-associated infections are one of the most frequent types
of adverse event to occur during care delivery and affect hundreds of
millions of patients worldwide every year.
4.
Pathophysiology
• INFECTION: Sepsisbegins with an infection caused by pathogens. this
can be systemic or localized.
• IMMUNE RESPONSE: The immune system detects the infection and
initiates an inflammatory response to fight the invading pathogens.
• INFLAMMATORY CASCADE: The immune response triggers a cascade
of inflammatory events, including the release of cytokines.
5.
Pathophysiology
• VASODILATION: Inflammatorycytokines cause blood vessels to
dilate.
• INCREASED CAPILLARY PERMEABILITY: The inflammatory
response can cause capillaries to become leaky,
• TISSUE EDEMA: The leaky capillaries result in tissue edema.
6.
Pathophysiology
• MICROCIRCULATORY DYSFUNCTION:In severe cases, the inflammatory
response can lead to dysfunction in the circulation, impairing the flow
of blood and oxygen to vital organs.
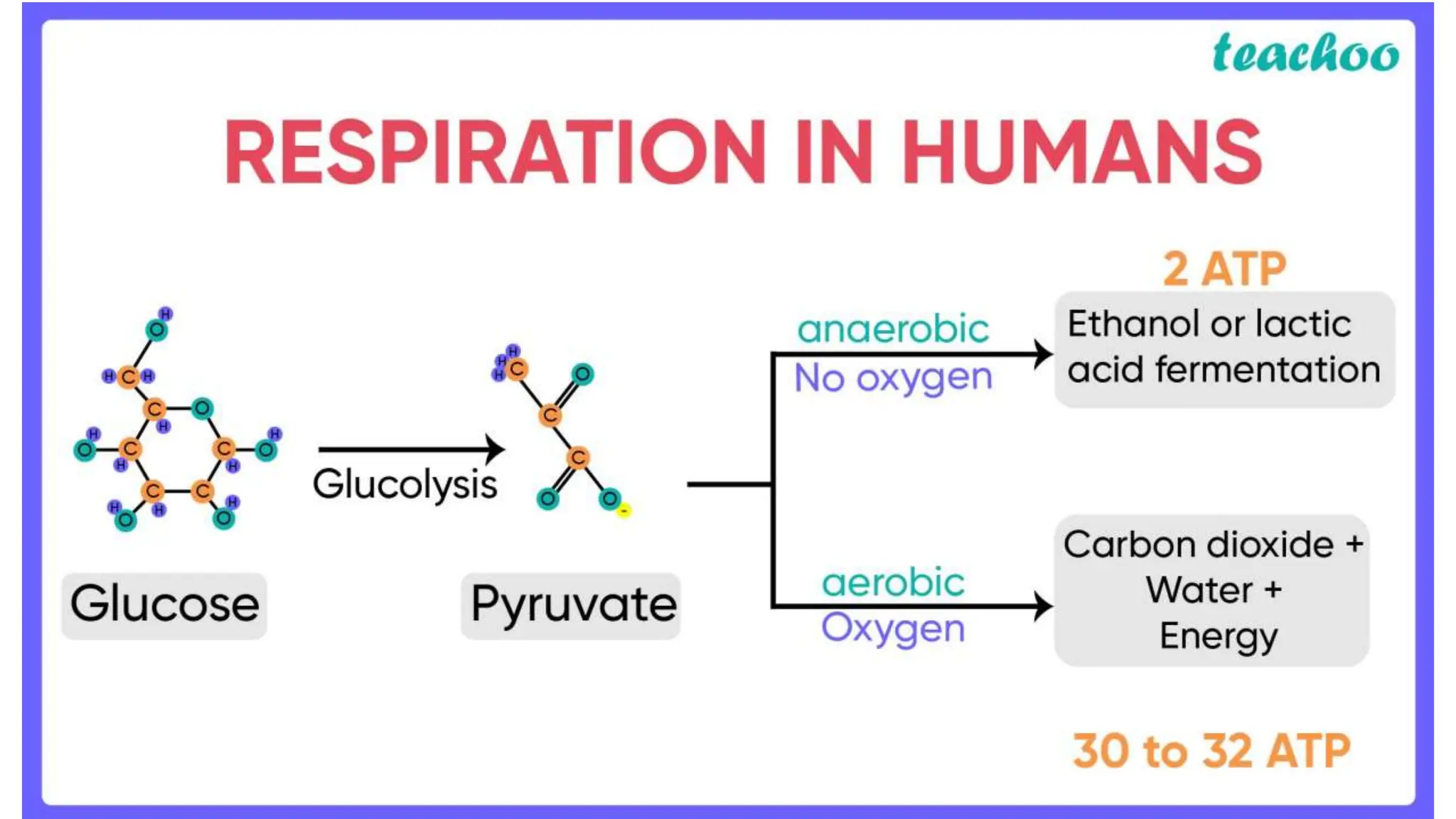
• METABOLIC SHIFT: As tissues become hypoxic (lack oxygen), they switch to
anaerobic metabolism, producing lactic acid.
• SYSTEMIC EFFECTS: The systemic inflammatory response can have
widespread effects on organs and systems throughout the body. This
can result in multi-organ dysfunction.
7.
Stages of thedisease
• SEPSIS: When the immune response to infection becomes dysregulated and
leads to widespread inflammation and organ dysfunction, it is referred
to as sepsis. (organ dysfunction can be identified as acute change in total
SOFA score> 2 points)
• SEPTIC SHOCK: Septic shock is the most severe stage, characterized by
extremely low blood pressure (hypotension unresponsive to fluid
replacement) and inadequate oxygen delivery to tissues. It is a medical
emergency. Mortality rate often exceed 50%.
• Clinically defined as sepsis with persisting hypotension requiring vasopressors to
maintain Mean Arterial pressure equal or more than 65mmHg and with serum lactate
more than 2mmol/L
8.
Common causes
• Bacterialinfections cause most cases of sepsis. Sepsis can also be a
result of other infections, including viral infections, such as COVID-19
or influenza, or fungal infections.
• diarrheal diseases (9.2 to 15 million annual cases)
• lower respiratory infections (1.8–2.8 million annually)
• non-communicable diseases are on the rise; one-third of sepsis cases
and nearly half of all sepsis-related deaths were due to an
underlying injury or chronic disease.
• Maternal disorders (most common non-communicable disease
complicated by sepsis)
9.
Common causes Amongchildren
• most common causes of sepsis-related deaths in children were
neonatal disorders.
• lower respiratory infections
• diarrheal diseases
• Group B streptococcus is the leading cause of both neonatal and
maternal sepsis.
• though E. coli is an emerging threat.
10.
Causative Agents
1.Gram-Positive Bacteria
•They currently account for nearly 50% of all sepsis cases,
• Ex:-Staphylococcus species, particularly Staphylococcus aureus, are frequently isolated. Notably, 14% of
cultures identify methicillin-resistant S. aureus (MRSA).
2.Gram-Negative Bacteria
• In the context of ICU infections, gram-negative bacteria cause 62% of cases.
• Ex- Pseudomonas species and Escherichia coli are prominent gram-negative pathogens linked
to sepsis.
3.Anaerobic Bacteria
• contribute to a smaller percentage of sepsis cases (around 4%).
• These bacteria are most frequently associated with intra-abdominal infections,
• representing 50%-70% of such cases.
• Ex:- Bacteroides fragilis, along with Peptostreptococcus and Clostridium species, are common anaerobic
culprits. B. fragilis infections are linked to a 20% increase in mortality and a 16-day longer hospital stay.
4.Fungi account for about 17% of sepsis cases.
Candida albicans is the leading fungus responsible for 13% of fungal-related sepsis
infections
11.
Risk factors
Anyone affectedby an infection, severe injury, or serious non-
communicable disease can progress to sepsis but vulnerable
populations are at higher risk including:
• older persons (65yrs or older)
• pregnant or recently pregnant women,
• neonates,
• hospitalized patients,
• patients in intensive care units,
• people with weakened immune systems (e.g. HIV, cancer)
• people with chronic medical conditions (e.g. kidney disease,
cirrhosis).
• People who survived sepsis.
12.
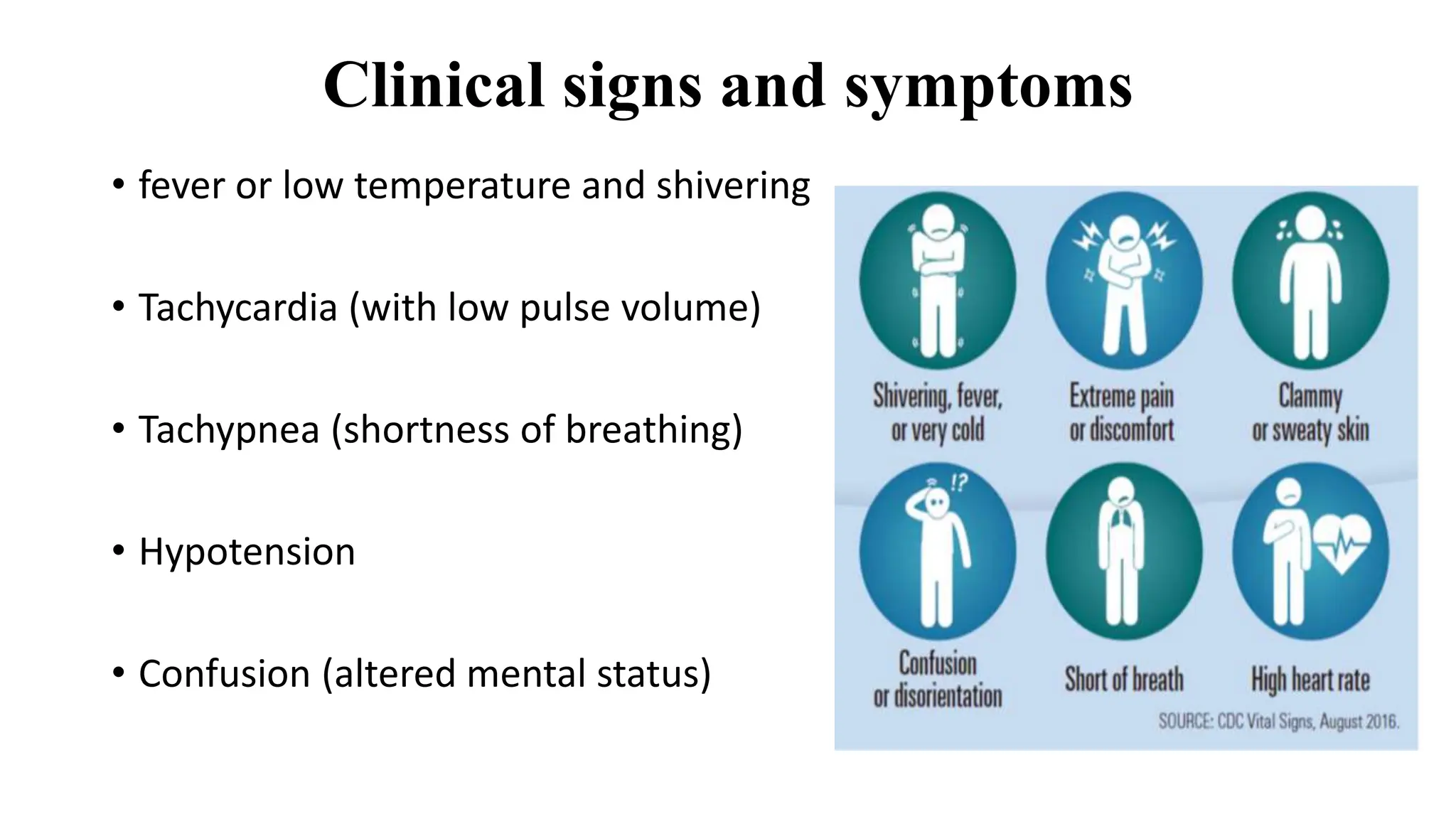
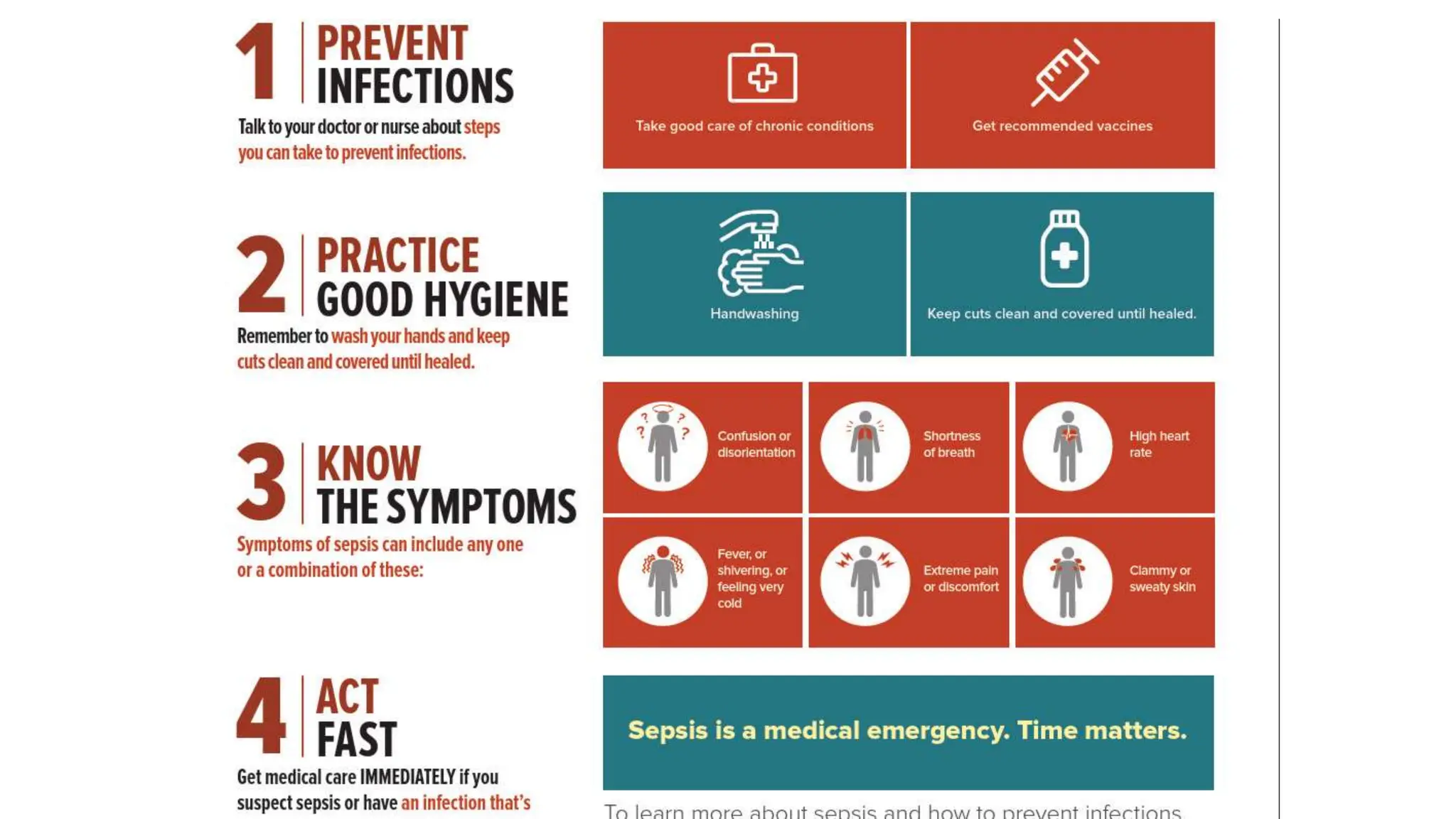
Clinical signs andsymptoms
• fever or low temperature and shivering
• Tachycardia (with low pulse volume)
• Tachypnea (shortness of breathing)
• Hypotension
• Confusion (altered mental status)
13.
Clinical signs andsymptoms
• clammy and sweaty skin with changed color.
• extreme body pain or discomfort.
• low urine output.
• Increased Lactate levels.
• Worsening organ functions.
• Suspected or confirmed infection.
14.
Symptoms in childreninclude
• fast breathing
• convulsions
• pale skin
• lethargy
• difficulty waking up
• feeling cold to the touch.
15.
Diagnostic criteria
• Sepsisis diagnosed through clinical signs and symptoms with
assessment findings. Consider all clinical information, including
assessments and lab results.
• Lactate Levels:
• Elevated lactate (>2 mmol/L) signifies tissue hypoxia and potential
sepsis.
• Serial lactate measurements are essential.
• Systemic inflammatory response syndrome (SIRS) is an exaggerated
defense response of the body to a noxious stressor (infection, trauma,
surgery, acute inflammation, ischemia or reperfusion or malignancy,)
• Earlier SIRS with a suspected source of infection is termed sepsis.
Confirmation of infection with positive cultures is therefore not
mandatory.
18.
Diagnostic criteria
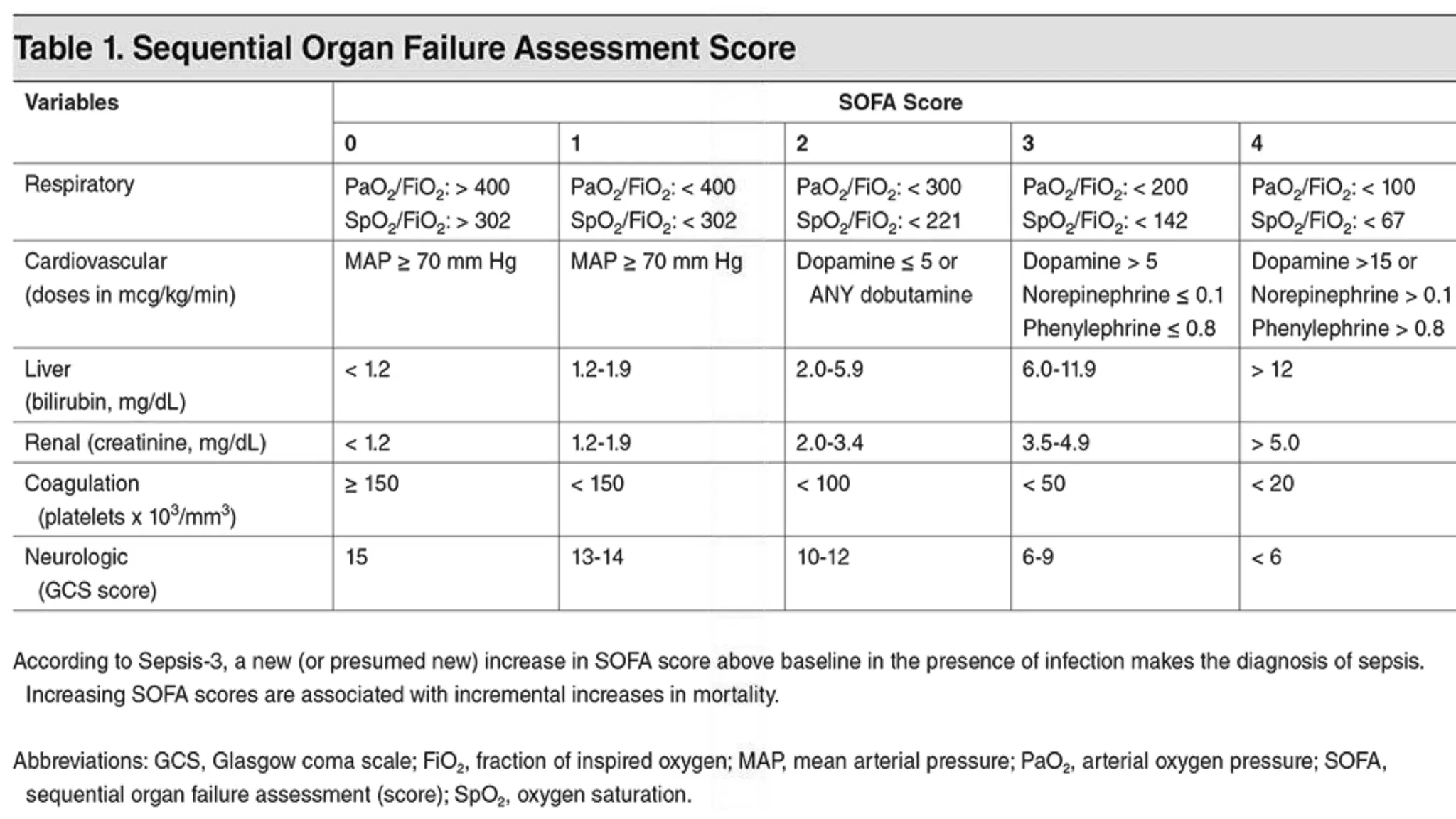
• SequentialOrgan Failure Assessment (SOFA)
• SOFA score assesses organ dysfunction.
• An increase by 2 or more points indicates sepsis.
• qSOFA helps identify high-risk patients outside the ICU.
• Criteria:
• Altered mental status,
• elevated respiratory rate,
• low blood pressure.
19.
SOFA (Sequential OrganFailure Assessment)
• It is a scoring system used by medical professionals to assess the severity
of a patient's organ dysfunction or failure.
• The SOFA score evaluates the functioning of several vital organs, including
the respiratory system, cardiovascular system, liver, coagulation system,
central nervous system, and renal system.
• SOFA scores are typically calculated at regular intervals during a patient's
hospital stay to track changes in organ function and guide clinical
management.
• Patients with a high SOFA score often have significant organ dysfunction
and may require intensive interventions. Such as mechanical ventilation for
respiratory failure, vasopressor support for cardiovascular instability,
dialysis for renal failure, and transfusions for coagulation abnormalities.
22.
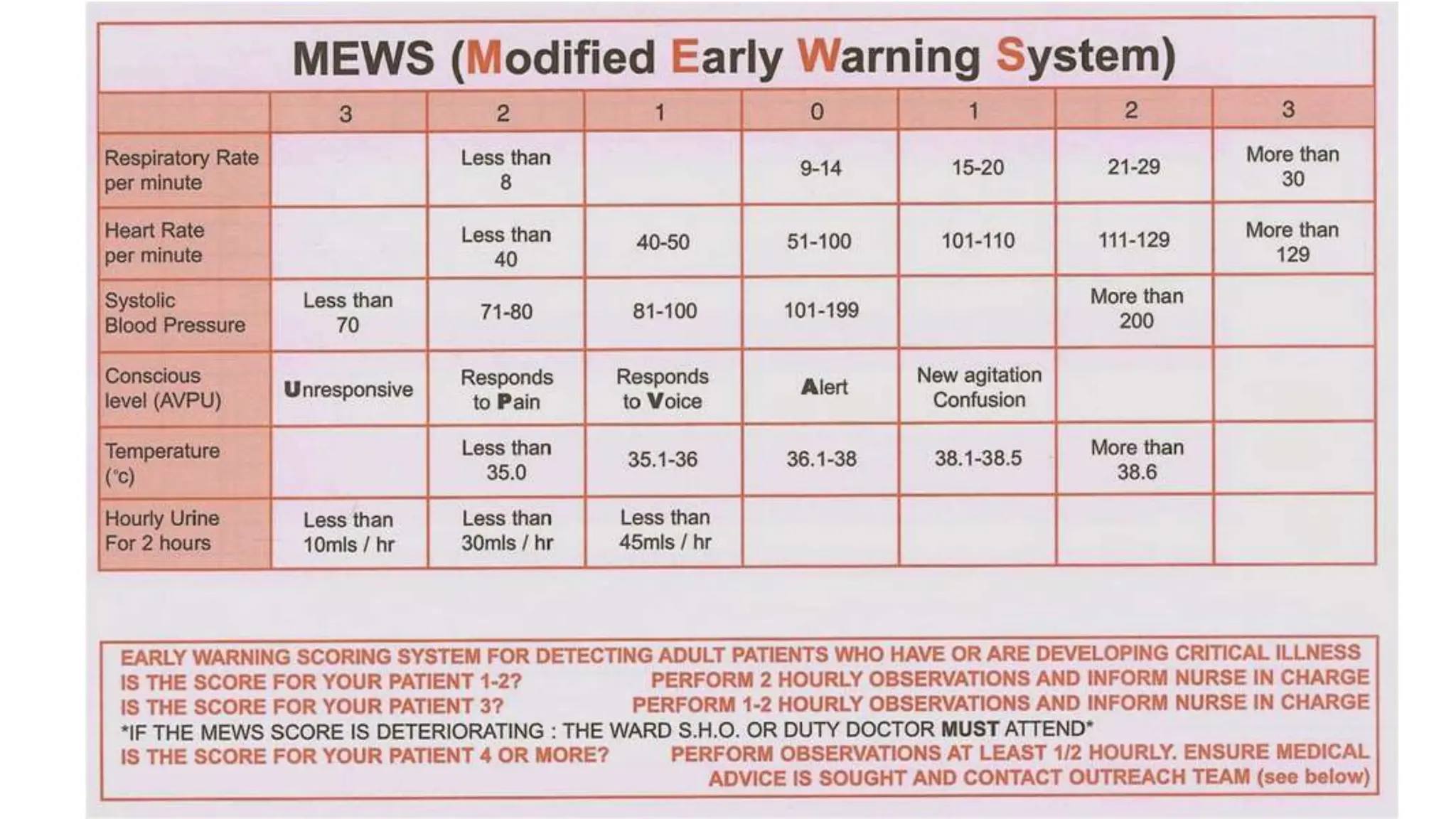
Modified Early WarningScore (MEWS)
• Early Warning System: MEWS (Modified Early Warning Score) is an early
warning system used in healthcare to monitor and detect early signs of
patient deterioration.
• Multiple Vital Signs: It assesses several vital signs like heart rate,
respiratory rate, blood pressure, temperature, consciousness level, and
oxygen saturation (if available) to create a comprehensive picture of a
patient's health.
• Timely Intervention: MEWS helps healthcare providers identify patients at
risk of worsening conditions, including sepsis, allowing for timely
interventions and potentially improving patient outcomes
Sepsis guideline (2021)suggestions
• For hospitals and health systems, we recommend using a
performance improvement program for sepsis, including
sepsis screening for acutely ill, high-risk patients and
standard operating procedures for treatment
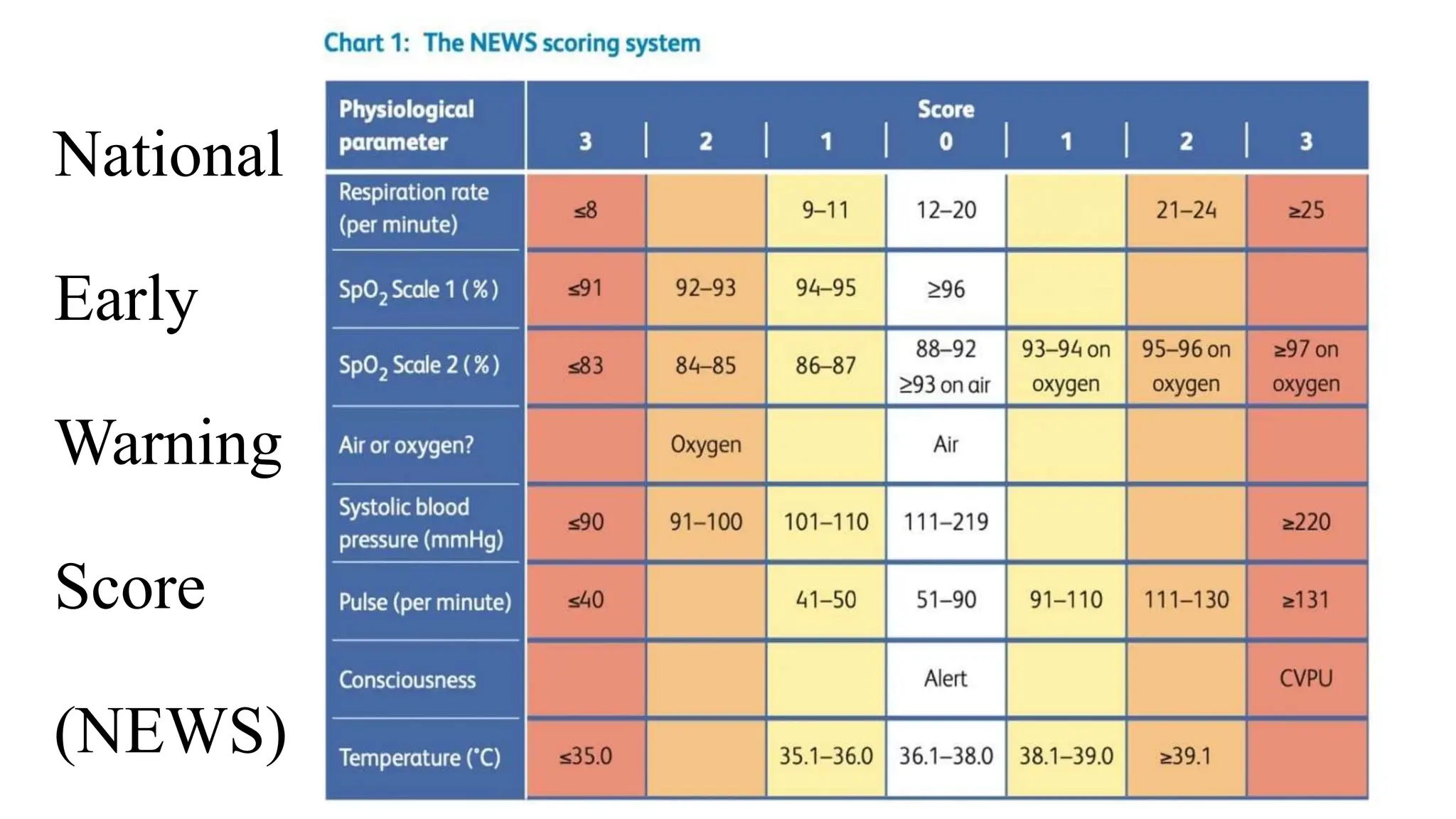
• We recommend against using qSOFA compared to SIRS,
NEWS, or MEWS as a single screening tool for sepsis or
septic shock
27.
Investigations
• Blood Cultures:Blood samples are collected from different sites to
identify the specific bacteria, fungi, or other pathogens causing the
infection.
• Full Blood Count (FBC): This test provides information about the
number and type of blood cells.
• Lactate Levels: Elevated lactate levels in the blood may indicate tissue
hypoxia, which is common in sepsis.
28.
Investigations
• Arterial BloodGas (ABG) or Venous Blood Gas (VBG): ABG or VBG
analysis helps evaluate the patient's acid-base balance, oxygenation
status, and respiratory function.
• Coagulation Profile: Assessing coagulation parameters can help
detect abnormalities associated with sepsis-induced coagulopathy.
• Renal Function Tests: Serum creatinine and blood urea nitrogen
(BUN) levels are monitored to assess kidney function. Acute kidney
injury is common in sepsis, and these tests help determine its
severity.
29.
Investigations
• Liver FunctionTests: Liver enzymes, such as alanine aminotransferase (ALT)
and aspartate aminotransferase (AST), are assessed to evaluate liver
function. Abnormalities may indicate sepsis-induced liver dysfunction.
• Electrolyte Levels: Measurement of electrolytes like sodium, potassium,
and chloride helps identify any imbalances that may occur during sepsis.
• Chest X-ray or CT Scan: Imaging studies may be ordered to identify the
source of infection, such as pneumonia, urinary tract infection, or an intra-
abdominal abscess.
30.
Investigations
• Urinalysis andUrine Culture: These tests can help diagnose urinary tract
infections (UTIs), which are a common source of sepsis, and determine the
causative pathogen.
• Cerebrospinal Fluid Analysis (if indicated): In cases of suspected central
nervous system involvement, a lumbar puncture may be performed to
analyze cerebrospinal fluid for signs of infection.
• Other Cultures: Depending on the clinical presentation, additional cultures
such as sputum cultures, wound cultures, or other relevant specimens may
be collected to identify the source of infection
31.
Elevated Lactic AcidLevels
• In sepsis, the body's response to infection can lead to widespread
inflammation and increased metabolic demands.
• As a result, oxygen delivery to tissues may become compromised
due to factors such as low blood pressure (hypotension) and
microvascular dysfunction.
• This can lead to tissue hypoxia (oxygen deprivation), which, in turn,
causes cells to switch from aerobic metabolism (utilizing oxygen for
energy) to anaerobic metabolism (producing energy without oxygen).
• During anaerobic metabolism, lactic acid accumulates in the tissues
and is released into the bloodstream, leading to elevated blood
lactate levels.
33.
Arterial Blood Gas(ABG) changes
During sepsis, both Arterial Blood Gas (ABG) and Venous Blood Gas (VBG) values can be affected.
Arterial Blood Gas (ABG) Changes:
• the pH can become acidic due to the accumulation of lactic acid and other metabolic
byproducts. This results in a decrease in pH (acidemia).
• PaO2 levels may decrease during sepsis. Hypoxemia can occur due to impaired lung function or
altered oxygen utilization in the tissues.
• PaCO2 (Partial Pressure of Carbon Dioxide): PaCO2 may be normal or decreased initially but can
increase later in sepsis, indicating impaired lung function and potential respiratory distress. In
some cases, patients with sepsis may develop septic shock, leading to respiratory failure and
increased PaCO2.
• HCO3- Bicarbonate levels may initially be normal or elevated as a compensatory response to
metabolic acidosis. However, as sepsis progresses, bicarbonate levels may decrease due to the
accumulation of lactic acid and the inability of the kidneys to fully compensate.
Hour-1 bundle: initialresuscitation for
sepsis and septic shock
1) Measure lactate level. *
2) Obtain blood cultures before administering antibiotics.
3) Administer broad-spectrum antibiotics.
4) Begin rapid administration of 30mL/kg crystalloid for
hypotension or lactate ≥4 mmol/L.
5) Apply vasopressors if hypotensive during or after fluid resuscitation
to maintain a mean arterial pressure ≥ 65 mm Hg.
• *Remeasure lactate if initial lactate elevated (> 2 mmol/L).
37.
International Guideline (2021)suggestions
1). Sepsis and septic shock are medical emergencies, and we
recommend that treatment and resuscitation begin
immediately.
2). For adults with sepsis or septic shock who require ICU
admission, we suggest admitting the patients to the
ICU within 6 h.
3). For adults with sepsis or septic shock, we recommend
prompt removal of intravascular access devices that
are a possible source of sepsis or septic shock after
other vascular access has been established.
38.
International Guideline suggestions
4).For adults with sepsis or septic shock, we recommend
initiating insulin therapy at a glucose level of ≥ 180
mg/dL (10 mmol/L)
5). Following initiation of an insulin therapy, a typical target
blood glucose range is 144–180 mg/dL (8–10 mmol/L)
6) For adults with possible septic shock or a high likelihood for
sepsis, we recommend administering antimicrobials
immediately, ideally within 1 h of recognition
39.
Fluid resuscitation
8).For patientswith sepsis induced hypoperfusion or septic
shock we suggest that at least 30 mL/kg of intravenous
(IV) crystalloid fluid should be given within the first 3 h
of resuscitation(according to clinical setting )
9) For adults with sepsis or septic shock, we recommend using
crystalloids as first-line fluid for resuscitation
10) Fluid resuscitation should be given only if patients present
with signs of hypoperfusion.
40.
Vasopressor therapy
11).For adultswith septic shock on vasopressors, we
recommend an initial target mean arterial pressure
(MAP) of 65 mmHg over higher MAP targets
12).For adults with septic shock, we recommend using
norepinephrine as the first-line agent over other
vasopressors.
13).For adults with septic shock on norepinephrine with
inadequate MAP levels, we suggest adding vasopressin
instead of escalating the dose of norepinephrine
Nursing assessment
• InitialEvaluation:
Begin with a thorough assessment upon admission or presentation.
• Vital Signs Monitoring:
• Continuously monitor temperature, heart rate, respiratory rate, blood pressure, and oxygen
saturation.
• Symptom Recognition:
• Be alert for early symptoms like fever, altered mental status, and malaise.
• Infection Source Identification:
• Determine the source of infection to guide diagnosis and treatment.
• Detailed History:
• Gather medical history, including recent infections, chronic illnesses, surgeries, and
immunosuppression.
• Physical Examination:
• Assess skin color, lung sounds, abdominal tenderness, and localized infection signs.
45.
Nursing assessment
• AssessmentTools:
• Use standardized criteria and scores for sepsis risk assessment.
• Laboratory and Diagnostic Tests:
• Order relevant tests, including blood counts, cultures, lactate levels, and imaging
studies.
• Mental Status Assessment:
• Evaluate consciousness, orientation, and signs of confusion.
• Fluid Balance Assessment:
• Monitor intake and output for fluid balance.
• Skin Assessment:
• Check for infection and perfusion issues.
• Neurological Assessment:
• Examine for neurological deficits indicating organ dysfunction.
46.
Nursing Diagnosis
Risk forInfection
• Goal: Prevent Infection
Interventions:
• Regularly assess for signs and symptoms of infections.
• Ensure hand hygiene compliance.
• Educate on infection prevention.
• Administer prophylactic antibiotics as medical order.
• Maintain sterile techniques while doing procedures.
47.
Nursing Diagnosis:
Risk forComplication related to Ongoing Sepsis or
Infection
• Goal: Prevention of Complications
• Interventions:
• Continuously monitor vital signs and clinical status.
• Administer prescribed antibiotics promptly.
• Provide intravenous fluids as ordered to maintain hemodynamic stability.
• Assess and manage pain and discomfort.
• Monitor for signs of organ dysfunction or septic shock.
• Collaborate with the healthcare team to adjust treatment as needed.
48.
Nursing Diagnosis:
Impaired GasExchange
• Goal: Optimize Oxygenation
Interventions:
• Administer oxygen as needed.
• Monitor respiratory status.
• Position for lung expansion.
• Teach deep breathing exercises.
• Administer respiratory medications.
• Manage mechanical ventilation.
49.
Nursing Diagnosis:
Decreased CardiacOutput
• Goal:To maintain the cardiac output
Interventions:
• Administer IV fluids and blood products.
• Monitor NIBP or central venous pressure.
• Give vasopressors as ordered.
• Monitor ECG and cardiac status.
• Maintain a calm environment.
• Address underlying causes.
Nursing Diagnosis:
Altered nutritionless than body requirement
• Goal: Improve the patient's nutritional status and support recovery.
• Interventions:
• Assess Patient: Comprehensive assessment: age, weight, medical history,
sepsis factors.
• Consult Dietitian: Develop personalized nutrition plan with patient's input.
• Monitor Intake & Output: Track food, fluids, urine, and drainage.
• Nutrition Support: Enteral or parenteral if oral intake insufficient.
• Frequent Small Meals: Promote digestion and prevent overload.
• Assist Feeding: Ensure comfort and support as needed.
• Dysphagia Check: Assess for swallowing difficulties and take precautions.
• Patient Education: Stress nutrition's role in recovery and guide adherence.
#5 Cytokinin = proteins that regulate immune responses
These cytokines signal immune cells to the infection site.
Vasodilatation leads to increased blood flow to the site of infection.
Capillary leaking allowing fluid, proteins, and immune cells to escape into the surrounding tissues.
#7 Elevated lactic acid levels indicate tissue hypoxia and can be measured in the blood.
Patients with sepsis often exhibit symptoms such as fever, increased heart rate, and altered mental status.
#8 Organ dysfunction such as kidney failure, respiratory failure, or coagulation abnormalities.
The term SEVERE SEPSIS was removed at 2016
Re-surviving sepis camp
#28 Multiple blood cultures are taken to increase the chances of identifying the pathogen.
Investigations explain කරන්න එපා
Elevated white blood cell (WBC) count, particularly an increase in immature forms (band cells), can indicate an infection.
#56 Thanks microbiology team kushlani jayathilaka madam and medical staff
Infection control nurse
Wd 06 sister and infection control nurse buddi miss
For giving us this valuble chance