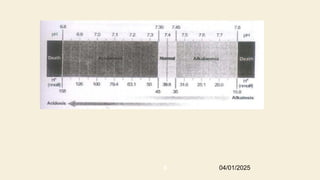
Basic concepts
● Acid-basedisorder; change in normal value of extracellular PH
that results when renal or respiratory function is abnormal or
when acid or base load over whelms excretory capacity.
● Acidemia-decrease in blood PH below normal range (<7.35)
• Acidosis-is process that increases H+
by increasing pco2 or
decreasing HCO3
−
● Alkalemia-elevation of blood PH above normal range(>7.45)
04/01/2025
3
Cont...
● Respiratory acidosis-A disorder that elevates PaCO2 & reduces PH
● Respiratory alkalosis- A disorder that reduces PaCO2 & elevates PH
● Metabolic acidosis- A disorder that reduces HCO-
3 & PH
● Metabolic alkalosis- A disorder that elevates HCO-
3 & PH
● Simple acid-base disorder- The presence of one of the above disorders with the
appropriate respiratory or renal compensation.
● Mixed acid-base disorder- The simultaneous presence of more than one acid-base
disorder.
04/01/2025
5
7
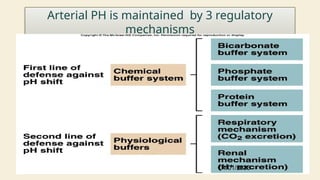
Arterial PH ismaintained by 3 regulatory
mechanisms
04/01/2025
8.
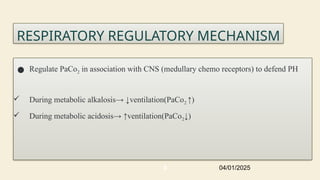
RESPIRATORY REGULATORY MECHANISM
●Regulate PaCo2 in association with CNS (medullary chemo receptors) to defend PH
During metabolic alkalosis→ ↓ventilation(PaCo2 ↑)
During metabolic acidosis→ ↑ventilation(PaCo2↓)
04/01/2025
8
9.
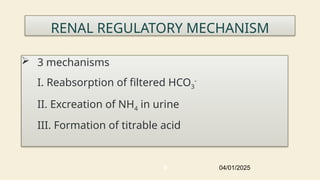
RENAL REGULATORY MECHANISM
3 mechanisms
I. Reabsorption of filtered HCO3
-
II. Excreation of NH4 in urine
III. Formation of titrable acid
04/01/2025
9
10.
ABG ANALYSIS
● ABGis a test that measures PH/PaCO2/PaO2/ SaO2/HCO3 concentration on
arterial blood
● Used for:-
○ Identification and monitoring of acid-base disturbances
○ Measurement of PaO2 and PaCO2
○ Assessment of the response to therapeutic interventions(eg, Insulin in
DKA)
○ Detection and quantification of the levels of abnormal hemoglobin
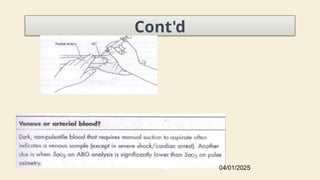
○ Procurement of a blood sample in an acute emergency when venous
sampling is not feasible.
04/01/2025
10
11.
Absolute
● An abnormalmodified
Allen's test
● Local infection or
distorted anatomy at
the puncture site,
● Severe peripheral
vascular disease of the
artery selected for
sampling
● Active Raynaud's
Relative
● Supra therapeutic
coagulopathy (INR
3, aptt 100
≥ ≥
seconds and
infusion of
thrombolytic agents
● A platelet count <50
x 109
Contraindications for ABG sampling
04/01/2025
11
Arterial Vs VenousGas Analysis
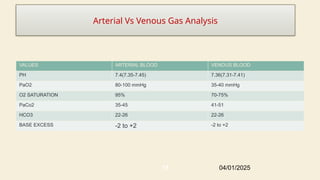
VALUES ARTERIAL BLOOD VENOUS BLOOD
PH 7.4(7.35-7.45) 7.36(7.31-7.41)
PaO2 80-100 mmHg 35-40 mmHg
O2 SATURATION 95% 70-75%
PaCo2 35-45 41-51
HCO3 22-26 22-26
BASE EXCESS -2 to +2 -2 to +2
04/01/2025
15
16.
Metabolic Acidosis
● Metabolicacidosis is defined as a pathologic process that, when
unopposed, increases the concentration of H+ in the body and reduces
HCO3.
○ ↓PH,↓HCo3,↓PaCo2
● Mechanisms
○ ↑ Acid production
○ Loss of bicarbonate
○ ↓ Renal acid excretion
○ Dilutional acidosis
04/01/2025
16
17.
Cont’d
● The serumanion gap can be used to categorize MA into two
groups
○ High anion gap MA
○ Normal anion gap MA
● Blood cations(+ve) must be balanced with anions(-ve) to
maintain electroneutrality
○ but when comparing main anions(Cl-,HCo3-) with main
cations (Na+,K+),there is shortage of anions this is termed
ANION GAP, which is 10-14(use 12 as absolute value)
04/01/2025
17
18.
Cont’d
● This gapis due to anions which are difficult to measure(SO4-, pO4-, -
vely charged proteins).
○ Anion Gap = Na - (Cl + HCo3)
○ Use 12 as an absolute value for AG
○ ↓1gm/dl albumin = add 2.5mmol to the Anion Gap
Corrected serum anion gap = (Serum anion gap measured) +
(2.5 x [4.5 - Observed serum albumin])
● An increase in the AG is most often due to an increase in
unmeasured anions and, less commonly, may be due to a decrease
in unmeasured cations (calcium, magnesium, potassium).
a serum potassium of 6 mEq/L will reduce the anion gap by 2 mEq/L
04/01/2025
18
19.
Special Scenarios
● Adecrease in the AG can be due to
1. The addition to the blood of abnormal cations,
2. A reduction in the plasma albumin
3. A decrease in the effective anionic charge on
albumin by acidosis;
4. Hyperviscosity and severe hyperlipidemia.
04/01/2025
19
22
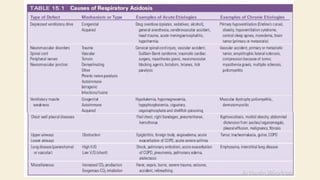
Clinical features
Profoundeffect on nervous, respiratory and cardiac system.
Depressed CNS (lethargy, stupor, coma), headache
Increased ventilation (Kussmaul breathing)
Depressed cardiac contractility but normal inotropic function due to
catecholamine release
Peripheral vasodilation, central vasoconstriction
Predisposed to pulmonary edema with minimal fluid due to low
pulmonary vasculature compliance
Glucose intolerance
04/01/2025
23.
Respiratory compensation
Thedevelopment of metabolic acidosis will normally
generate a compensatory respiratory response
With normal respiratory compensation, Pco2
decreases by 1.2 mm Hg for every 1 mEq/L net
decrease in [HCO3–].
04/01/2025
23
24.
Cont’d
PCO2 =(1.5 x HCO3 + 8) ± 2.
This equation, which is called Winter’s formula, was
derived in children, half of whom were between
two months and two years of age.
PCO2 = HCO3 + 15.
The PCO2 should approximate the decimal digits of the
arterial pH.
04/01/2025
24
25.
Cont….
These ruleswork well for mild to moderately severe
metabolic acidosis (HCO3 between 7 and 22 mEq/L).
For more severe metabolic acidosis (HCO3 less than 7
mEq/L), the pCO2 should be maximally reduced to the 8
to 12 mmHg range.
As an example: pH = 7.30; pCO2 = 30 mmHg (4.0 kPa);
04/01/2025
25
26.
The delta aniongap/ delta HCO3 ratio in high
anion gap MA
When the AG increases in magnitude as a result of
metabolic acidosis, that increase should be compared
with the magnitude of the fall in HCO3.
This represents the delta AG/delta HCO3 ratio.
Opposite changes in the serum AG and
HCO3 concentration would result in a
delta AG/delta HCO3 ratio of 1:1
04/01/2025
26
27.
Cont'd
A deltaAG/delta HCO3 ratio below 1 suggests one of the
following:
A coexisting normal AG metabolic acidosis .
A high AG acidosis in which both renal function is
preserved and the acid anion is readily excreted into
the urine
Patients with renal tubular acidosis of early renal
insufficiency
A delta AG/delta HCO3 ratio of 1:1 is consistent with an
04/01/2025
27
28.
Cont'd
A deltaAG/delta HCO3 ratio between 1 and 2 generally
occurs with
high AG metabolic acidosis, such as lactic acidosis,
when renal function is reduced and the acid anions
are, thereby, all retained in the body.
Metabolic alkalosis coexists with a high AG
metabolic acidosis or
When the baseline HCO3 level is elevated as a
result of chronic respiratory acidosis.
04/01/2025
28
29.
Cont'd
● Delta AG/deltaHCO3 ratio above 2 usually suggests
that metabolic alkalosis coexists with a high AG
metabolic acidosis or that the baseline HCO3 level is
elevated as a result of chronic respiratory acidosis.
04/01/2025
29
30.
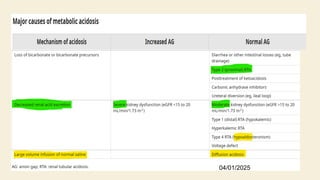
Renal vs Extrarenalcauses of MA
Renal and extrarenal causes of metabolic acidosis can be
distinguished by measuring urinary ammonia excretion.
Because most laboratories do not measure urinary
ammonia,
one can indirectly assess ammonia excretion by measuring
the urinary anion gap (UAG).
04/01/2025
30
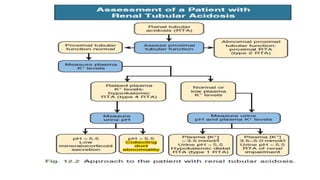
Renal tubular acidosis
In RTA metabolic acidosis develops because of defects
in the ability of the renal tubules to perform the
normal functions required to maintain acid-base
balance.
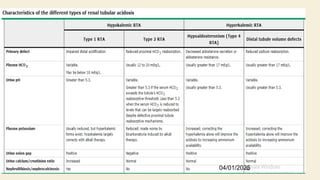
All forms of RTA are characterized by a normal anion
gap (hyperchloremic) metabolic acidosis.
04/01/2025
32
Treatment of MA
●General approach
○ Reverse the underlying pathophysiologic mechanism
○ General vs specific approach
○ Consider acute and chronic forms of MA separately
● Acute MA
○ Alkali therapy
■ Severe acidemia with pH<7.1
■ pH 7.1-7.2 with severe acute kidney injury (ie, a twofold or
greater increase in serum creatinine or oliguria)
04/01/2025
35
Chronic MA
Themost common causes of chronic metabolic acidosis are diarrhea,
advanced chronic kidney disease, and the various forms of RTA
Alkali therapy
Consider benefits of therapy
The rational for alkali therapy is summarized here:
Increasing the bicarbonate concentration reduces or eliminates the
need for compensatory hyperventilation and can alleviate the
dyspnea experienced by some patients.
Chronic metabolic acidosis may have adverse effects on muscle
function and metabolism, skeletal integrity, hormone levels, and
other physiologic parameters. In children, for example, correction of
chronic metabolic acidosis restores skeletal growth
04/01/2025
37
38.
Cont…
Patients withchronic distal (type 1) RTA are likely to develop
nephrocalcinosis and calcium-containing kidney stones. This
defect can be reversed with adequate bicarbonate
replacement.
Chronic metabolic acidosis in patients with kidney dysfunction
may accelerate the progression of their kidney damage, and
reversal of the acidosis can slow this process
04/01/2025
38
39.
Dosing of alkalitherapy (when given)
● Ampules of hypertonic sodium bicarbonate are available as 8.4 percent
(50 mEq/50 mL), 7.5 percent (44.6 mEq/50 mL), and 4.2 percent solutions
(25 mEq/50 mL).
Acute metabolic acidosis
● The initial goal is a pH >7.2 and/or serum bicarbonate concentration >16
mEq/L.
● Infuse 2 ampules (100 mL) of 7.5 percent sodium bicarbonate (44.6
mEq/50 mL) over 1 to 2 minutes and remeasure the blood pH and serum
bicarbonate concentration (eg, after two hours).
● If the distribution space is approximately 55 percent of the body weight
(as it is in healthy individuals), the serum bicarbonate level should increase
by approximately 2 to 3 mEq/L.
04/01/2025
39
40.
Cont..
Chronic metabolicacidosis – When chronic alkali treatment is
required, options include the sodium or potassium salts of either
bicarbonate or a metabolizable anion such as citrate or lactate
The potassium salts are indicated when hypokalemia and total body
potassium deficits exist. In general, the initial dose is 50 to 100 mEq
per day, which is then titrated up, or down, as required.
If ongoing bicarbonate losses persist or accelerate, the dose will need
to be adjusted accordingly
04/01/2025
40
41.
Cont’d
Treatment goal
Increase[HCO3] to 10-12mmol/L and the PH to 7.20
● Preferred alkali is NaHCO3
○ HCO3 deficit= HCO3 space * HCO3 deficit/L
○ HCO3 space= (0.4 + (2.6/HCO3)) * lean body
weight
04/01/2025
41
42.
42
Lactic Acidosis
Lactateis an end product in glucose metabolism
Formed by reduction of pyruvate catalyzed by LDH
Principal sites of production are skeletal muscle (25%), skin (25%), red blood
cells (20%), brain (20%), and intestine (10%).
Activated neutrophils are an additional source of lactate in inflammatory
conditions like ARDS
The concentration of lactate in plasma is usually 2 mmol/L, with a
lactate:pyruvate ratio of 10:1
Lactate is cleared from plasma by the liver (60%), kidneys (30%), and heart
(10%).
04/01/2025
43.
43
Lactic Acidosis
● Themost common cause of metabolic acidosis in
hospitalized patients
● Lactate level >2mmol/L –hyperlactatemia
● Lactate level > 4mmol/L – lactic acidosis
● D-Lactic acid acidosis – formed by gut bacteria
● L-lactic acid acidosis
○ Type A
○ Type B
04/01/2025
44.
44
Type A –hypoxic (Poor tissue perfusion)
● Circulatory insufficiency (septic/hypovolemic shock,
heart failure, mesenteric ischemia)
● Severe anemia
● Mitochondrial enzyme deficiency
● Inhibitors (carbon monoxide, cyanide)
04/01/2025
45.
45
Type B –non hypoxic (aerobic disorders)
● Severe infections
(malaria, cholera)
● Renal failure
● Hepatic failure
● Seizure
● Thiamine deficiency
Drugs/toxins
● NRTIs
● Metformin – primarily in
renal insufficiency. Treated
with dialysis
● Isoniazid
● Fructose
● Acetaminophen depletes
glutathione
pyroglutamic acidemia in
critical illness
● Ethanol, methanol,
propylene glycol
04/01/2025
46.
46
L-Lactic acidosis treatment
●Correct underlying cause.
● Restore tissue perfusion
● Alkali therapy for severe, acute academia
○ Alkali therapy if indicated(Severe acidemia (PH<7.00) to improve cardiovascular
function.)
Therapeutic goal
● To raise arterial PH to no more than 7.2 or the [HCO3] to no more than 12meq/L over
30-40mins
○ HCO3 not an effective buffer unless pH is very low
○ NaHCO3 may worsen acidosis by stimulating lactate production
(phosphofructokinase)
○ Overshoot alkalosis (lactate is converted to bicarbonate)
○ It is a CO2 burden that must be removed by the lungs. Carbicarb is a commercially
available buffer solution that is a 1:1 mixture of sodium bicarbonate and disodium
04/01/2025
47.
Cont’d
● DKA= standardDKA mx
● Alcoholic ketoacidosis
○ Fluid replacement therapy with saline and 5% dw
○ Corection of electrolyte disturbance
● GI bicarbonate loss
○ Treat the cause
○ Volume replacement and alkali therapy when indicated
04/01/2025
47
48.
Reverse/prevents
● Reduced leftventricular
contractility
● Arrhythmias
● Arterial vasodilation
● Impaired responsiveness to
catecholamine
Potential harms of
bicarbonate therapy
● Increased arterial and tissue
capillary PCO2
● Acceleration of lactate
generation
● Reduced ionized calcium
● Hypernatremia
● Extracellular fluid volume
expansion
Benefits of HCO3
therapy
04/01/2025
48
49.
Cont’d
● CKD
○ Currentlythe 2013 Kidney Disease Improving Global Outcomes (KDIGO)
guidelines recommended that, in patients with CKD and metabolic
acidosis, alkali therapy be used to maintain the [HCO3] in the normal
range (23 to 29 meq/L).
○ Renal replacemnt therapy
● RTA
○ Maintenance of normokalemia
○ Alkali therapy with sodium and potassium citrate
○ Mineralocorticoid therapy
○ Diuretic therapy
04/01/2025
49
50.
Classic distal RTA
●Administration of NaHCO3 or sodium citrate with a goal of correcting the
HCO3 to normal level.
● Concomitant administration of potassium in acutely acidotic patients
with hyopkalemia.
● Alkali therapy decrease frequency of nephrocalcinosis, improve bone
density and resume normal growth pattern in children.
Generalized distal RTA
● Restore normokalemia.
04/01/2025
50
51.
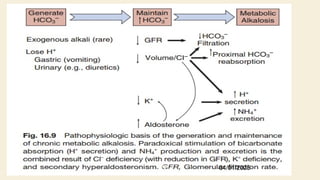
Metabolic Alkalosis
Metabolicalkalosis is caused by retention of
excess alkali and is characterized by
↑PH, HCo3, PaCo2
↑ ↑
Hypoventilation, producing a secondary increase
in arterial Pco2.
04/01/2025
51
52.
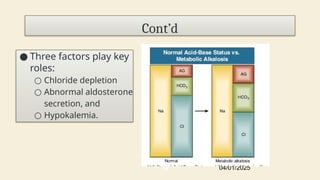
● Three factorsplay key
roles:
○ Chloride depletion
○ Abnormal aldosterone
secretion, and
○ Hypokalemia.
04/01/2025
52
Cont’d
Features
● The mostimportant adverse effect is
hypokalemia,which increase the likelihood of cardiac
arrythmia(esp. in pts with underlying cardiac dysfunction)
● Usually pts with Hco3 level up to 40mmol/l can be
assymptomatic but when > 50 mmol/l may develop
seizures,tetany,delirium or stupor.
04/01/2025
57
58.
Respiratory compensation
● ThePCO2 raises by 0.7mmHg for every 1mEq/L elevation
in serum HCO3 concentration
○PCO2=HCO3 + 10
○PCO2 = 40 + 0.7 × ([HCO3 ] 24)
−
04/01/2025
58
59.
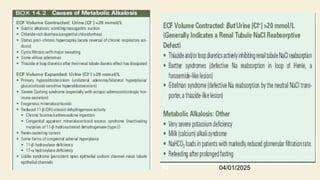
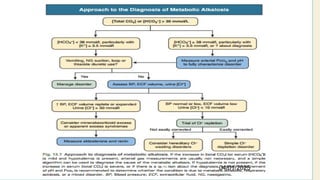
Diagnosis
● Diagnosis ofmetabolic alkalosis involves three steps.
● The first step
○ Detection, is most often based on the finding of elevated
venous [total CO2].
● The second step
○ evaluation of the secondary response (hypoventilation), excluding the possibility that a
respiratory acid-base abnormality is also present.
○ This step requires measurement of arterial pH and Pco2.
● The third step
○ Determination of the cause
04/01/2025
59
60.
Cont’d
●Serum [total CO2]levels above 30
mmol/l in association with
hypokalemia are virtually
pathognomonic of metabolic
alkalosis.
04/01/2025
60
Treatment
What isthe cause of excessive serum HCO3
concentration?
Why is the excess HCO3 not excreted through
the urine?
04/01/2025
62
63.
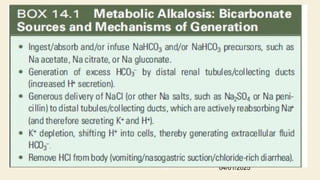
Treating factors thatincrease HCO3 production
GI H+ loss
- PPIs or H2-blockers
- Reduce gastric suctioning
Intracellular H+ shift
- Correction of hypokalemia
Exogenous alkali administration
- Discontinue all alkali including Na+ and K+ salts of any organic
anion that will later be metabolized to HCO3
Excessive Renal H+ loss
- Discontinue diuretics.
04/01/2025
63
64.
Treating factors thatimpair renal excretion
of HCO3
1. Reduced arterial blood volume
True volume depletion
● Can be caused by vomiting, NGT suctioning, diuretic
use, blood loss, loss of blood into 3rd
space and marked
sweat loss(CF).
● Corrected by volume expansion by isotonic saline
● Treatment of concomitant hypokalemia
04/01/2025
64
65.
Cont’d
Reduced effective arterialblood volume (edematous state)
● Metabolic alkalosis occur due to diuretic therapy and
hypokalemia as complication of diuretic therapy.
● Volume replacement has no role.
● Acetazolamide is the preferred diuretics.
○ Carbonic anhydrase inhibitor.
○ Dose = 125-250 mg po daily or twice daily.
○ Mechanism – inhibit proximal NaHCO3 reabsorption and
increase HCO3 excretion.
○ Exacerbates hypokalemia.
04/01/2025
65
66.
Cont’d
2. Chloride depletion
●Volume expansion with chloride containing salts
3. Potassium depletion
● Correction of Hypokalemia with Potassium chloride.
4. Renal failure
● Hemodialysis against a dialysate low in [HCO3] and
high in [Cl–
] can be effective when renal function is
impaired.
04/01/2025
66
67.
Cont’d
Which group ofpatients are treated with HCL?
Severe metabolic alkalosis (HCO3 >50meq/l
or PH>7.55.
Pts with renal insufficiency who can’t be
dialyzed.
04/01/2025
67
68.
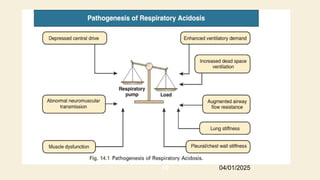
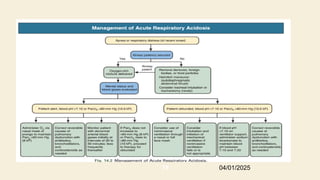
RESPIRATORY ACIDOSIS
• Respiratoryacidosis is the acid-base disturbance initiated by an
increase
in CO2 tension (Pco2) of body fluids and whole-body CO2 stores
• The level of PaCO2 is determined by the of two factors, the rate of
carbon dioxide production (VCO2) and the rate of alveolar ventilation
(VA)
• Its main elements are the respiratory pump, which generates a
pressure gradient responsible for airflow, and the loads that oppose
such action.
• CO2 retention can occur from an imbalance between the strength of
04/01/2025
68
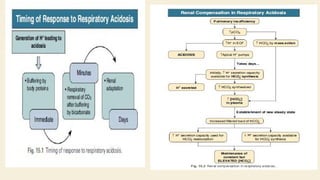
Secondary physiologic response
●Inacute respiratory acidosis, there is a compensatory elevation in
HCO3
−
(due to cellular buffering mechanisms) that increases 1 mmol/L
for every 10-mmHg increase in Paco2.
●In chronic respiratory acidosis (>24 h), renal adaptation increases the
04/01/2025
72
73.
Chronic adaptation renalregulation
mechanisms
It requires 3-5 days of sustained hypercapnia for
completion.
A transient increase in urinary net acid excretion
persistent ,increase in the rate of renal bicarbonate
reabsorption
plasma HCO3
- ↑0.4 mEq/L for each mm Hg chronic
increment in PaCO2; 04/01/2025
73
74.
Clinical presentation
Variesaccording to the severity and duration of respiratory acidosis, the
underlying disease, and whether there is accompanying hypoxemia.
Systemic vasodilalatation (most obvious in cerebral circulation, direct
relation to the level of Paco2)
CO2 retention (whether acute or chronic) is always associated with
hypoxemia in patients breathing room air.
04/01/2025
74
Diagnosis
● ABG analysis;↑PaCO2 (>45 mmhg)arterial pH <7.35
↓
● A detailed history and physical examination may
indicate the cause.
● For pulmonary causes, pulmonary function studies
including spirometry, diffusion capacity for CO, lung
volumes and arterial Paco2 and O2 saturation
● For non-pulmonary causes, a detailed drug history,
measurement of hematocrit, and assessment of
upper airway, chest wall, pleura and neuromuscular
04/01/2025
76
77.
TREATMENT Respiratory Acidosis
Dependson its severity and rate of onset
Reverse the underlying cause and alveolar ventilation
Oxygen administration
Ventilatory Support (NIPPV vs invasive)
Avoide aggressive and rapid correction of hypercapnia
provide sufficient Cl and K+ to enhance the renal
−
excretion of HCO3 .
−
04/01/2025
77
RESPIRATORY ALKALOSIS
Respiratoryalkalosis is the acid-base
disturbance initiated by a reduction in PaCO2.
Develops when a sufficiently strong ventilatory
stimulus causes CO2 output in the lungs to
exceed its metabolic production by the tissues.
It is the most common acid-base
abnormality in critically ill patients
Is an adverse prognostic sign, especially
if Paco2 is below 20 to 25 mm Hg
04/01/2025
80
81.
Secondary physiologic response/adaptation
○The compensatory response to acute respiratory
alkalosis reduces the HCO3 conc. by 2 meq/l for
every 10 mmhg decline in the PCO2
○If the reduced PCO2 persists for more than 3-5
days, then the disorder is considered chronic &
the serum HCO3 conc. should fall by 4-5 meq/l for
every 10 mmhg reductin in the PCO2
04/01/2025
81
Clinical manifestation
• Dependsthe severity and duration but
primarily underlying disease.
1. Neurological: Rapid decrements in PaCO2 to half
the normal values or lower are typically
accompanied by
paresthesias of the extremities,
chest discomfort,
circumoral numbness, lightheadedness,
confusion, and infrequently, tetany or generalized
seizures. These manifestations are seldom present in
04/01/2025
83
84.
cardiovascular
No appreciablechanges in CO,BP or cardiac
rhythm occur in actively hyperventilating subjects.
major reductions in cardiac output and blood
pressure, and substantial hyperlactatemia frequently
occur in passively hyperventilating ( MV ).
patients with CAD might suffer hypocapnia-induced
coronary vasoconstriction, resulting in angina
pectoris and arrhythmias.
04/01/2025
84
85.
Diagnosis
●ABG analysis ↑PH(7.45) PCO2 < 35 mmhg
↓ ↓
HCO3
-
●patient history, physical examination, and
ancillary laboratory
●Plasma K + is often reduced and the Cl- is
increased.
04/01/2025
85
86.
Treatment
● The managementof respiratory alkalosis is directed toward alleviation
of the underlying disorder.
● Respiratory alkalosis usually occurs in response to some stimulus,
treatment is usually unsuccessful unless the stimulus is controlled.
● Avoid rapid correction vasodilation of ischemic areas, resulting in
→
reperfusion injury in the brain & lung.
● Mechanically ventilated patients adjust tidal volume rate, sedation
and pain control
04/01/2025
86
Mixed ABD
Refersto the presence of two or more
independent acid base disorders.
Evaluation of ABD initially require identification
of the major disorder and determination of the
degree of compensation
Inappropriate compensation suggests a second
04/01/2025
88
To check forcompensation
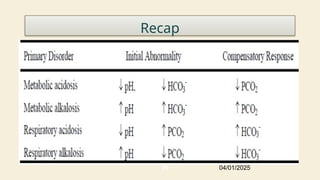
Primary Disorder Expected Compensation pH
Metabolic Acidosis Winter’s Formula
pCO2 = 1.5 [HCO3] + 8 +/- 2
Metabolic Alkalosis Summer’s Formula
pCO2 = 0.7 [HCO3] + 20 +/- 5
Respiratory Acidosis
Acute
[HCO3] rises by 1 for every 10 mm Hg increase in pCO2 Expect pH decrease 0.08 for every 10 mmHg
increase in PCO2
Chronic [HCO3] rises by 4 for every 10 mm Hg increase in pCO2 Expected pH do decrease 0.03 for every 10 mmHg
increase in PCO2
Respiratory Alkalosis
Acute
[HCO3] decreases by 2 for every 10 mm Hg decrease in pCO2 Expect pH increase 0.08 for every 10 mmHg
decrease in PCO2
Chronic [HCO3] decreases by 5 for every 10 mm Hg decrease in pCO2 Expected pH to increase 0.02 for every 10 mmHg
decrease in pCO2
04/01/2025
90
91.
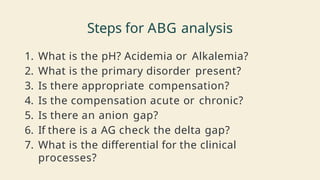
Steps for ABGanalysis
1. What is the pH? Acidemia or Alkalemia?
2. What is the primary disorder present?
3. Is there appropriate compensation?
4. Is the compensation acute or chronic?
5. Is there an anion gap?
6. If there is a AG check the delta gap?
7. What is the differential for the clinical
processes?
92.
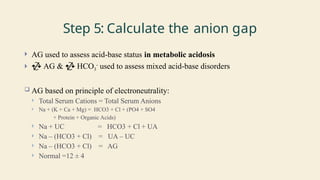
Step 5: Calculatethe anion gap
AG used to assess acid-base status in metabolic acidosis
AG & HCO3
-
used to assess mixed acid-base disorders
AG based on principle of electroneutrality:
Total Serum Cations = Total Serum Anions
Na + (K + Ca + Mg) = HCO3 + Cl + (PO4 + SO4
+ Protein + Organic Acids)
Na + UC = HCO3 + Cl + UA
Na – (HCO3 + Cl) = UA – UC
Na – (HCO3 + Cl) = AG
Normal =12 ± 4
93.
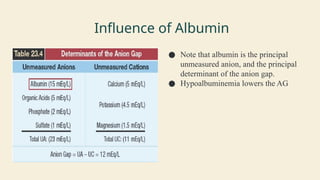
Influence of Albumin
●Note that albumin is the principal
unmeasured anion, and the principal
determinant of the anion gap.
● Hypoalbuminemia lowers the AG
94.
Cont...
The AGcan be adjusted for low albumin levels by using the following formula
AG corrected = AG + 2.5[4 – albumin]
(4 represents the normal concentration of albumin in plasma).
If there is an anion Gap then calculate the Delta/delta gap (step 6) to determine
additional hidden nongap metabolic acidosis or metabolic alkalosis
If there is no anion gap then start analyzing for non-anion gap acidosis
Step6:CalculateDeltaGap
● The delta-delta
●The ratio of ΔAG/Δ[HCO3]
● Used in anion gap metabolic acidosis.
● This would reveal additional METABOLIC disorder.
● You can have an anion gap metabolic acidosis
○ Plus a non-AG metabolic acidosis
○ OR
○ Plus a metabolic alkalosis!
97.
Delta-Delta
● The ratioof ΔAG/Δ[HCO3].
■ AG-normal AG/ normal [HCO3] – [HCO3]
● Using 12 as normal AG, and 24 as normal [HCO3]
■ AG-12/24- [HCO3]
● If ratio of ΔAG/Δ[HCO3] is….
○ >2 : metabolic alkalosis is present.
○ 1-2: no other metabolic disorder.
○ <1: additional non-anion gap metabolic acidosis
98.
Delta-delta made simple
●Step 1: calculate the ΔAG
● Step 2: add the ΔAG to the current [HCO3-]
● Step 3: compare this new [HCO3-] to the normal range of 22-28.
○ <22additional non-AG metabolic acidosis is present
○ >28additional metabolic ALKALOSIS is present.
○ 22-28: no additional metabolic disorder
Answer
The patienthas high Ph- alkalemia
The pco2 is high(respiratory acidosis) and the
bicarbonate is high
(metabolic alkalosis)
The high Ph and high bicarbonate tell us the
metabolic alkalosis is the primary process
The AG-10,normal value
Summary:a primary metabolic alkalosis with
respiratory compensation
04/01/2025
100
Answer
The patienthas a low pH
The patient has a high pco2(respiratory
acidosis) and a high bicarbonate (metabolic
alkalosis).
The combination of low pH and high pco2
tells us that the respiratory acidosis is the
primary process
Summary: primary respiratory acidosis with
compensatory metabolic alkalosis
04/01/2025
102
answer
The patienthas a very low pH(acidemia)
The patient has a low pcow(respiratory alkalosis) and a
very low bicarbonate (metabolic acidosis).
The low pH in conjunction with the low bicarbonate
tells us the metabolic acidosis is the primary process
The AG is elevated at 30- high AG MA
The respiratory alkalosis is the compensatory
process,although despite a huge increase in Minute
ventilation the patient still has a very low ph
04/01/2025
104
105.
Cont…
The deltagap is 30-12=18 and the delta
delta is 18+2=20.
since the delta delta is below 22,we know
that there is additional non gap metabolic
acidosis as well
Summary: combined elevated anion gap
and non gap metabolic acidosis with
compensatory respiratory alkalosis
04/01/2025
105
Answer
The patienthas a low pH(acidemia)
The pco2 is low ((respiratory alkalosis) and the bicarbonate is
low(metabolic acidosis)
The combination of low pH and the low bicarbonate tells us that the
metabolic acidosis is the primary process
The anion gap is elevated at 24.This tells us the patient has a primary
high AG MA
The delta gap is 24-12=12. The delta delta is 12+17=29.because the Del-
Del is greater than 26,we know the patient has a concurrent metabolic
alkalosis
Summary: Primary elevated anion gap metabolic acidosis with
respiratory compensation and a concurrent metabolic alkalosis
04/01/2025
107
108.
Case 3
● 42year old man experienced crushing substernal
chest pain and diaphoresis and shortness of breath
and was brought to the emergency room.
○ Vital signs: BP 70/50 HR 110 RR 14
○ Arterial blood gas analysis on room air:
○ pH 7.32/PCO2 24 mmHg/PO2 88 mm Hg/ HCO3ֿ 12
mEq/l /SaO2 96%
● Serum electrolytes:
○ Na 135 mEq/l K 5.4 mEq/l Cl 101 mEq/l , Lactate 12
mEq/l
04/01/2025
108
109.
Answer
• Acidosis
• Metabolicacidosis
• Over-compensated
• High anion gap
• Delta/delta <1
• Respiratory alkalosis ans aditional non anaion gap acidosis
• Primary high anion gap metabolic acidosis with secondary
repiratory alkalosis and aditional non anion gap
metabolic acidosis
04/01/2025
109
#3 Acidemia (as opposed to acidosis) is defined as a low arterial pH (<7.35), which can result from a metabolic acidosis, respiratory acidosis, or both
#9 Renal excretion of acid involves the combination of hydrogen ions with urinary titratable acids, particularly phosphate (HPO42- + H+ → H2PO4-), and ammonia to form ammonium (NH3 + H+ → NH4+) [1]. The latter is the primary adaptive response since ammonia production from the metabolism of glutamine can be appropriately increased in response to an acid load
#13 Acute rather than chronic hypocalcemia is seen in critically ill
patients or as a consequence of certain medications and often does
not require specific treatment. Transient hypocalcemia is seen with
severe sepsis, burns, acute kidney injury, and extensive transfusions
with citrated blood.
#16 Dilution acidosis — Dilution acidosis refers to a fall in serum bicarbonate concentration that is primarily due to rapid infusion of large volumes of normal saline, which contains neither bicarbonate nor the sodium salts of organic anions that can be metabolized to bicarbonate (such as lactate or acetate)
#17 The normal anion gap metabolic acidoses must, by definition, manifest relative hyperchloremia (a high chloride relative to the sodium concentration).
#18 The serum anion gap falls by approximately 2.5 mEq/L for every 1 g/dL (10 g/L) reduction below normal (4.5 g/dL) in the serum albumin concentration
Thus, a serum potassium of 6 mEq/L will reduce the anion gap by 2 mEq/L.
Marked hypercalcemia and/or hypermagnesemia can similarly reduce the anion gap.
Another cause of a reduced or negative anion gap is immunoglobulin G (IgG) multiple myeloma
#20 D-lactic acidosis – D-lactic acid is generated by bacterial fermentation of ingested, but unabsorbed, carbohydrates. D-lactic acidosis results from excessive absorption of D-lactic acid from the lumen of the gastrointestinal tract, usually in patients with jejunoileal bypass or short bowel syndrome.
#21 When urine is exposed to gastrointestinal mucosa, which occurs after ureteral implantation into the sigmoid colon or the creation of replacement urinary bladder using a segment of the gastrointestinal tract
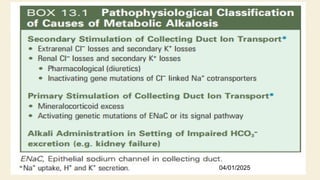
Distal (type 1) RTA and type 4 RTA, in which tubular dysfunction is the primary problem and glomerular filtration is initially preserved
#23 In all simple acid-base disorders, the primary abnormality generates a compensatory response that results in both the HCO3 concentration and pCO2 moving in the same direction (either both will increase or both will decrease)
This respiratory response to metabolic acidosis begins within 30 minutes and is complete by 12 to 24 hours.
#24 The pCO2 should approximate the decimal digits of the arterial pH. As an example, if the pH is 7.25, then the pCO2 should be approximately 25 mmHg
#25 This is consistent with a simple metabolic acidosis with appropriate respiratory compensation; all three of the compensation rules presented above are satisfied
An inability to generate an appropriate hyperventilatory response is generally indicative of a significant underlying neurologic or respiratory disorder and represents a mixed acid-base disorder: metabolic acidosis and respiratory acidosis. Conversely, excessive hyperventilation, which reduces the pCO2 below the expected range, is indicative of mixed metabolic acidosis and respiratory alkalosis
#34 Similar considerations apply when hydrogen ions are retained because of impaired renal acid excretion due to distal (type 1) or type 4 RTA or hypoaldosteronism. In these conditions, a normal anion gap acidosis develops since there is no retention of unmeasured anions
#35 Severe and symptomatic acute acidemia can most rapidly be treated by the intravenous administration of sodium bicarbonate. Despite its potential adverse effects, sodium bicarbonate remains the most frequently used alkalinizing agent
#45 NRTI – inhibition of mitochondrial DNA polymerase
Propylene glycol – solvent in lorazepam, diazepam, phenytoin
Fructose competitively inhibits conversion of glycogen to glucose leading to lactic acidosis
Isoniazid toxicity causes seizures and lactic acidosis
#49 CKD-Previously, sodium bicarbonate therapy was not recommended. (fear of volume expansion and hypertension)
Proximal RTA
Administration of alkali result in increase urinary excretion of potassium
Combination of sodium and potassium citrate should be administered.
#68 The ventilatory system is responsible for maintaining eucapnia by adjustment of alveolar minute ventilation (V ̇ A) to match the rate of CO2 production.
An increase in arterial pCO2 can occur by one of three possible mechanisms:
Presence of excess CO2 in the inspired gas
Decreased alveolar ventilation
Increased production of CO2 by the body
#80 This occurs when there is excessive loss of CO2 by hyperventilation of lungs.
#83 Acute hypocapnia causes cerebral vasoconstriction and decreases cerebral blood flow (in severe cases it can reach values less than 50% of normal) but flow essentially normalizes during sustained hypocapnia.
#86 Respiratory alkalosis itself is rarely life threatening.
Therefore, emergent treatment is usually not indicated unless the pH level is greater than
7.5
If the PaCO2 is corrected rapidly in patients with chronic respiratory alkalosis, metabolic acidosis may develop due to the renal compensatory drop in serum bicarbonate. respiratory alkalosis usually occurs in response to some stimulus, treatment is usually unsuccessful unless the stimulus is controlled
#92 This is usually equal to 12 ± 4 meq/L and is usually due to the negatively charged plasma proteins as the charges of the other unmeasured cations and anions tend to balance out.
When acid is added to the body, the [H+] increases and the [HCO3-] decreases. In addition, the concentration of the anion, which is associated with the acid, increases. This change in the anion concentration provides a convenient way to analyze and help determine the cause of a metabolic acidosis by calculating what is termed the anion gap.
#99 Explanation for the clinical picture: The patient has hypercalcemia and a
metabolic alkalosis. In conjunction with a clinical history of heavy milk and
calcium carbonate consumption, these abnormalities suggest the patient is
suffering from milk-alkali syndrome. In response to metabolic alkaloses, patients
develop hypoventilation. This explains his elevated PCO2and respiratory acidosis that, in turn, explains his hypoxemia
#101 Explanation for the clinical picture: The patient has very severe COPD and chronic carbon dioxide retention. As a result, you expect that at baseline, they will have a chronic respiratory acidosis (his baseline PCO2was 58) with a compensatory metabolic alkalosis. In this case, the clinical history suggests the patient is in an exacerbation. When the patient presents to the ER, his PCO2is elevated above his baseline. Because this is an acute change, the bicarbonate has not had time to adjust and the pH falls. This case is, therefore, an example of an respiratory acidosis
#103 Case 4 Explanation for the clinical picture: The patient has concurrent elevated anion gap and non-gap acidoses with respiratory compensation. The acidoses are so severe that, despite the high minute ventilation, the pH remains very low. This patient has a history of inhalant abuse and one of the commonly abused inhalants, toluene, can present with severe elevated anion gap acidosis with respiratory compensation. The severe elevated anion gap acidosis is due to accumulation of one of the main toluene metabolites, hippuric acid
#106 Explanation for the clinical picture: A history of epigastric pain, nausea and vomiting in conjunction with elevated lipase and amylase on laboratory studies is consistent with the diagnosis of pancreatitis. As a result of the pancreatitis, the patient has developed an elevated anion gap acidosis with respiratory compensation. The concurrent metabolic alkalosis is likely due to vomiting, which eads to hydrogen ion loss via the upper gastrointestinal tract.

![Cont’d
● This gap is due to anions which are difficult to measure(SO4-, pO4-, -
vely charged proteins).
○ Anion Gap = Na - (Cl + HCo3)
○ Use 12 as an absolute value for AG
○ ↓1gm/dl albumin = add 2.5mmol to the Anion Gap
Corrected serum anion gap = (Serum anion gap measured) +
(2.5 x [4.5 - Observed serum albumin])
● An increase in the AG is most often due to an increase in
unmeasured anions and, less commonly, may be due to a decrease
in unmeasured cations (calcium, magnesium, potassium).
a serum potassium of 6 mEq/L will reduce the anion gap by 2 mEq/L
04/01/2025
18](https://image.slidesharecdn.com/abg-250401185917-4cd20d1c/85/Seminar-on-acid-base-disorders-nephrolog-18-320.jpg)

![Respiratory compensation
The development of metabolic acidosis will normally
generate a compensatory respiratory response
With normal respiratory compensation, Pco2
decreases by 1.2 mm Hg for every 1 mEq/L net
decrease in [HCO3–].
04/01/2025
23](https://image.slidesharecdn.com/abg-250401185917-4cd20d1c/85/Seminar-on-acid-base-disorders-nephrolog-23-320.jpg)
![Cont’d
Treatment goal
Increase [HCO3] to 10-12mmol/L and the PH to 7.20
● Preferred alkali is NaHCO3
○ HCO3 deficit= HCO3 space * HCO3 deficit/L
○ HCO3 space= (0.4 + (2.6/HCO3)) * lean body
weight
04/01/2025
41](https://image.slidesharecdn.com/abg-250401185917-4cd20d1c/85/Seminar-on-acid-base-disorders-nephrolog-41-320.jpg)
![46
L-Lactic acidosis treatment
● Correct underlying cause.
● Restore tissue perfusion
● Alkali therapy for severe, acute academia
○ Alkali therapy if indicated(Severe acidemia (PH<7.00) to improve cardiovascular
function.)
Therapeutic goal
● To raise arterial PH to no more than 7.2 or the [HCO3] to no more than 12meq/L over
30-40mins
○ HCO3 not an effective buffer unless pH is very low
○ NaHCO3 may worsen acidosis by stimulating lactate production
(phosphofructokinase)
○ Overshoot alkalosis (lactate is converted to bicarbonate)
○ It is a CO2 burden that must be removed by the lungs. Carbicarb is a commercially
available buffer solution that is a 1:1 mixture of sodium bicarbonate and disodium
04/01/2025](https://image.slidesharecdn.com/abg-250401185917-4cd20d1c/85/Seminar-on-acid-base-disorders-nephrolog-46-320.jpg)
![Cont’d
● CKD
○ Currently the 2013 Kidney Disease Improving Global Outcomes (KDIGO)
guidelines recommended that, in patients with CKD and metabolic
acidosis, alkali therapy be used to maintain the [HCO3] in the normal
range (23 to 29 meq/L).
○ Renal replacemnt therapy
● RTA
○ Maintenance of normokalemia
○ Alkali therapy with sodium and potassium citrate
○ Mineralocorticoid therapy
○ Diuretic therapy
04/01/2025
49](https://image.slidesharecdn.com/abg-250401185917-4cd20d1c/85/Seminar-on-acid-base-disorders-nephrolog-49-320.jpg)

![Respiratory compensation
● The PCO2 raises by 0.7mmHg for every 1mEq/L elevation
in serum HCO3 concentration
○PCO2=HCO3 + 10
○PCO2 = 40 + 0.7 × ([HCO3 ] 24)
−
04/01/2025
58](https://image.slidesharecdn.com/abg-250401185917-4cd20d1c/85/Seminar-on-acid-base-disorders-nephrolog-58-320.jpg)
![Diagnosis
● Diagnosis of metabolic alkalosis involves three steps.
● The first step
○ Detection, is most often based on the finding of elevated
venous [total CO2].
● The second step
○ evaluation of the secondary response (hypoventilation), excluding the possibility that a
respiratory acid-base abnormality is also present.
○ This step requires measurement of arterial pH and Pco2.
● The third step
○ Determination of the cause
04/01/2025
59](https://image.slidesharecdn.com/abg-250401185917-4cd20d1c/85/Seminar-on-acid-base-disorders-nephrolog-59-320.jpg)
![Cont’d
●Serum [total CO2] levels above 30
mmol/l in association with
hypokalemia are virtually
pathognomonic of metabolic
alkalosis.
04/01/2025
60](https://image.slidesharecdn.com/abg-250401185917-4cd20d1c/85/Seminar-on-acid-base-disorders-nephrolog-60-320.jpg)
![Cont’d
2. Chloride depletion
● Volume expansion with chloride containing salts
3. Potassium depletion
● Correction of Hypokalemia with Potassium chloride.
4. Renal failure
● Hemodialysis against a dialysate low in [HCO3] and
high in [Cl–
] can be effective when renal function is
impaired.
04/01/2025
66](https://image.slidesharecdn.com/abg-250401185917-4cd20d1c/85/Seminar-on-acid-base-disorders-nephrolog-66-320.jpg)
![To check for compensation
Primary Disorder Expected Compensation pH
Metabolic Acidosis Winter’s Formula
pCO2 = 1.5 [HCO3] + 8 +/- 2
Metabolic Alkalosis Summer’s Formula
pCO2 = 0.7 [HCO3] + 20 +/- 5
Respiratory Acidosis
Acute
[HCO3] rises by 1 for every 10 mm Hg increase in pCO2 Expect pH decrease 0.08 for every 10 mmHg
increase in PCO2
Chronic [HCO3] rises by 4 for every 10 mm Hg increase in pCO2 Expected pH do decrease 0.03 for every 10 mmHg
increase in PCO2
Respiratory Alkalosis
Acute
[HCO3] decreases by 2 for every 10 mm Hg decrease in pCO2 Expect pH increase 0.08 for every 10 mmHg
decrease in PCO2
Chronic [HCO3] decreases by 5 for every 10 mm Hg decrease in pCO2 Expected pH to increase 0.02 for every 10 mmHg
decrease in pCO2
04/01/2025
90](https://image.slidesharecdn.com/abg-250401185917-4cd20d1c/85/Seminar-on-acid-base-disorders-nephrolog-90-320.jpg)
![Cont...
The AG can be adjusted for low albumin levels by using the following formula
AG corrected = AG + 2.5[4 – albumin]
(4 represents the normal concentration of albumin in plasma).
If there is an anion Gap then calculate the Delta/delta gap (step 6) to determine
additional hidden nongap metabolic acidosis or metabolic alkalosis
If there is no anion gap then start analyzing for non-anion gap acidosis](https://image.slidesharecdn.com/abg-250401185917-4cd20d1c/85/Seminar-on-acid-base-disorders-nephrolog-94-320.jpg)
![Case
Calculate Anion gap
• ABG :PH 7.23/ PCO217/ HCO-
3 7
• BMP: Na 123/ Cl 97/BUN 119/ Cr 5.1/Albumin 2
AG = Na – Cl – HCO3 (normal 12 ± 4)
○ 123 – 97 – 7 = 19
AG corrected = AG + 2.5[4 – albumin]
● = 19 + 2.5 [4 – 2]
● = 19 + 5 = 24](https://image.slidesharecdn.com/abg-250401185917-4cd20d1c/85/Seminar-on-acid-base-disorders-nephrolog-95-320.jpg)
![Step6:CalculateDeltaGap
● The delta-delta
● The ratio of ΔAG/Δ[HCO3]
● Used in anion gap metabolic acidosis.
● This would reveal additional METABOLIC disorder.
● You can have an anion gap metabolic acidosis
○ Plus a non-AG metabolic acidosis
○ OR
○ Plus a metabolic alkalosis!](https://image.slidesharecdn.com/abg-250401185917-4cd20d1c/85/Seminar-on-acid-base-disorders-nephrolog-96-320.jpg)
![Delta-Delta
● The ratio of ΔAG/Δ[HCO3].
■ AG-normal AG/ normal [HCO3] – [HCO3]
● Using 12 as normal AG, and 24 as normal [HCO3]
■ AG-12/24- [HCO3]
● If ratio of ΔAG/Δ[HCO3] is….
○ >2 : metabolic alkalosis is present.
○ 1-2: no other metabolic disorder.
○ <1: additional non-anion gap metabolic acidosis](https://image.slidesharecdn.com/abg-250401185917-4cd20d1c/85/Seminar-on-acid-base-disorders-nephrolog-97-320.jpg)
![Delta-delta made simple
● Step 1: calculate the ΔAG
● Step 2: add the ΔAG to the current [HCO3-]
● Step 3: compare this new [HCO3-] to the normal range of 22-28.
○ <22additional non-AG metabolic acidosis is present
○ >28additional metabolic ALKALOSIS is present.
○ 22-28: no additional metabolic disorder](https://image.slidesharecdn.com/abg-250401185917-4cd20d1c/85/Seminar-on-acid-base-disorders-nephrolog-98-320.jpg)