Outline of
the
presentation
Introduction
Normal ABG Values
Determine acid - base disorders
Metabolic Acidosis
Metabolic Alkalosis
Respiratory Acidosis
Respiratory Alkalosis
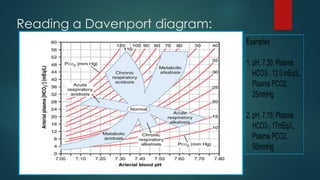
Reading a Davenport diagram
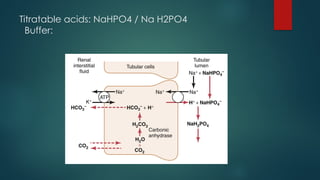
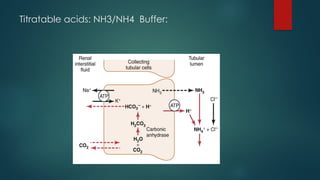
Titratable acids
Mixed disorders
Delta Ratio
Clinical Vignettes
Q & A
3.
Introduction:
pH= -log10 [H+]
[H+]ions are precisely regulated by the body at 37–43 neq/L with arterial blood having a normal pH range of 7.35
to 7.45(7.4+ 0.05), abnormal pH leads to physiological and biochemical changes with sometimes fatal
consequences.
Major ICF ( intra cellular fluid) buffers:
Proteins : Important intracellular buffers Hemoglobin
H+ + HbO2 HHb + O2
Organic phosphates (ATP, AMP, ADP)
(60–70% of buffering occurs inside cells)
Major ECF( extra cellular fluid) buffers:
Bicarbonate : Is the most important ECF buffer in blood plasma
* H2O + CO2 H2CO3 H+
+ HCO3
−
Phosphate-biphosphate : Is important renal tubular buffering
HPO4− + H+ H2PO4 −
Ammonia : Also, important renal tubular buffering
NH3 + H+ NH4 +
4.
Henderson –Hasselbalch Equation
pH = -log [H+] ~ 6.1( pKa) + log [HCO3-] / (0.03)(pCO2) pKa = 6.1
Titration Curve for Bicarbonate Buffer System
The carbon-dioxide/bicarbonate buffer is the most important buffer in extracellular fluid even though the
concentration of the components are low and pKa of the system is 6.1, which is not very close to normal
extracellular fluid pH (7.4).
Reason: To maintain a pH 7.4 the components of the system
(CO2 and HCO3−) are closely regulated by the lungs and the
Kidneys, respectively.
5.
What are somecommon causes to H+ ions changes in ECF:
1. Volatile Acid: Carbonic acid produced from cellular respiration
2. Non-volatile acid: Inorganic and organic acids, Sulfuric Acid, Phosphoric Acid, Keto acids
(protein metabolism)
3. Muscular Activity → Lactic Acid
4. GI Absorption food ingestion
5. GI secretions leaving the body: Gastric Vomiting → Lose H+ ions
Diarrhea → Lose Bicarbonate ions
6. Urinary Losses
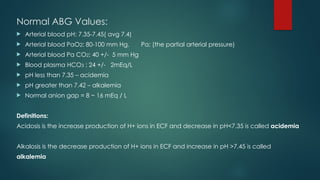
Normal ABG Values:
Arterial blood pH: 7.35-7.45( avg 7.4)
Arterial blood PaO2: 80-100 mm Hg, Pa: (the partial arterial pressure)
Arterial blood Pa CO2: 40 +/- 5 mm Hg
Blood plasma HCO3 : 24 +/- 2mEq/L
pH less than 7.35 – acidemia
pH greater than 7.42 – alkalemia
Normal anion gap = 8 − 16 mEq / L
Definitions:
Acidosis is the increase production of H+ ions in ECF and decrease in pH<7.35 is called acidemia
Alkalosis is the decrease production of H+ ions in ECF and increase in pH >7.45 is called
alkalemia
8.
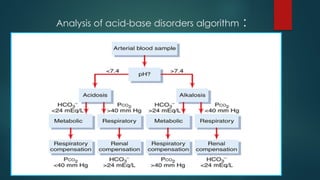
Determine acid -base disorders:
CO2 + H2O *carbonic anhydrase H2CO3 H+ + HCO3- *pH= [HCO3-] / (pCO2)
Step 1: Look at the pH to determine acidotic or alkalotic condition
Step 2: Look at the levels of PaCO2 and HCO3 to determine primary disorder
If the change in HCO3 is consistent with change in pH ,then it is a metabolic disorder
If the change in Pa CO2 is consistent with change in pH, then it is a respiratory disorder
Step 3: look to see if there is another primary disorder
Compensation for respiratorydisorders:
CO2 + H2O H2CO3 H+ + HCO3- in the presence of
*carbonic anhydrase
Compensation in renal is slow takes hours to days to respond:
Acidosis – increase H+ secretion – increased HCO3- reabsorption
Alkalosis – decreased H+ secretion – incomplete HCO3- reabsorption resulting in decreased
plasma HCO3-
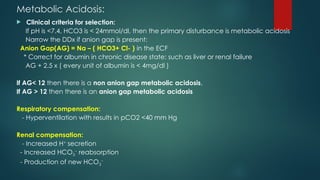
Metabolic Acidosis:
Clinicalcriteria for selection:
If pH is <7.4, HCO3 is < 24mmol/dl, then the primary disturbance is metabolic acidosis
Narrow the DDx if anion gap is present:
Anion Gap(AG) = Na – ( HCO3+ Cl- ) in the ECF
* Correct for albumin in chronic disease state: such as liver or renal failure
AG + 2.5 x ( every unit of albumin is < 4mg/dl )
If AG< 12 then there is a non anion gap metabolic acidosis,
If AG > 12 then there is an anion gap metabolic acidosis
Respiratory compensation:
- Hyperventilation with results in pCO2 <40 mm Hg
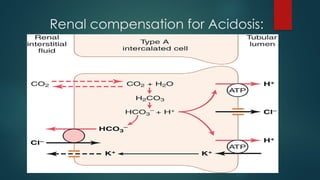
Renal compensation:
- Increased H+
secretion
- Increased HCO3
−
reabsorption
- Production of new HCO3
−
16.
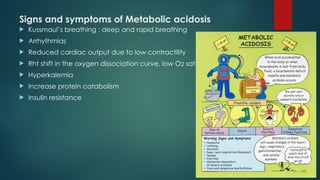
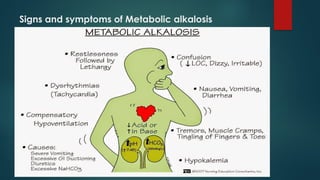
Signs and symptomsof Metabolic acidosis
Kussmaul’s breathing : deep and rapid breathing
Arrhythmias
Reduced cardiac output due to low contractility
Rht shift in the oxygen dissociation curve, low O2 sat
Hyperkalemia
Increase protein catabolism
Insulin resistance
17.
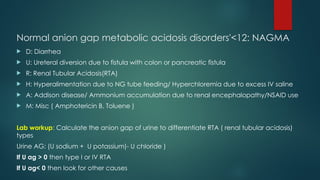
Normal anion gapmetabolic acidosis disorders'<12: NAGMA
D: Diarrhea
U: Ureteral diversion due to fistula with colon or pancreatic fistula
R: Renal Tubular Acidosis(RTA)
H: Hyperalimentation due to NG tube feeding/ Hyperchloremia due to excess IV saline
A: Addison disease/ Ammonium accumulation due to renal encephalopathy/NSAID use
M: Misc ( Amphotericin B, Toluene )
Lab workup: Calculate the anion gap of urine to differentiate RTA ( renal tubular acidosis)
types
Urine AG: (U sodium + U potassium)- U chloride )
If U ag > 0 then type I or IV RTA
If U ag< 0 then look for other causes
18.
Increase anion gapmetabolic acidosis disorders: AG>12:
AGMA
M : Methanol toxicity
U: Uremia from renal failure
D: Diabetic ketoacidosis
P: Para-aldehyde
I: Ischemia / Isoniazid / Iron
L: Acidosis due to lactic acid
E: Ethylene Glycol
R: Rhabdomyolysis
S : Starvation / Salicylate poisoning
Initial Lab workup:
Serum levels : ketones, salicylate, toxicology screen, ck levels
19.
Metabolic Alkalosis:
Criteriafor selection:
If pH is >7.4, HCO3 is > 24mmol/dl, then the primary disturbance is metabolic alkalosis
Causes:
Severe gastric vomiting / NG suction
Hyper mineralocorticoid states( Conn’s syndrome)
Over diuresis or abuse with Furosemide or Hydrochlorothiazide
Lab workup: Urine chloride levels to differentiate volume depletion
Urine chloride <10: Indicates volume depletion, severe gastric vomiting, diuresis abuse/
NG tube use
Urine chloride >10: Indicates licorice use, hypomagnesaemia, Bartter’s syndrome
Respiratory compensation( fast) : Hypoventilation PCO2 rises 0.5-1 for each unit increase in HCO3-
from a baseline of 24
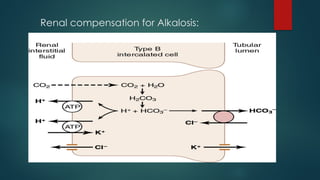
Renal compensation( slow): Decreased H+ secretion, Decreased HCO3− reabsorption
Loss of HCO3− in urine
Respiratory Acidosis:
Criteriafor selection:
If pH is <7.4, pCO2 is > 40 mm Hg, then the primary disturbance is respiratory acidosis
develop due to hypoventilation causing decrease CO2 clearance
Causes:
Chest cavity: Neuromuscular disorder, pneumothorax, pleural effusion
Central respiratory drive: CNS depression, Sedation, Opioid O/D, sleep apnea,
hypoventilation
Issue with lungs: Pneumonia, pulmonary edema, reactive airway diseases( COPD),
tumor
Renal compensation for respiratory acidosis:
Acute respiratory acidosis: for every pCO2 increase of 10, HCO3 increase by 1 with pH
decrease by 0.08
Chronic respiratory acidosis: for every Pco2 increase of 10, HCO3 increase by 3-4 with
pH decrease by 0.03
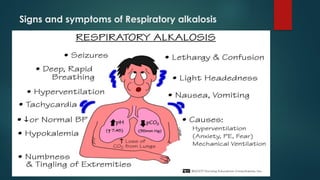
Respiratory Alkalosis:
Criteriafor selection:
If pH is >7.4, pCO2 is < 40 mm Hg, then the primary disturbance is respiratory alkalosis
develop due to hyperventilation causing increase CO2 clearance
Causes:
Systemic: Sepsis, Salicylate O/D, liver failure, CHF
Central: Ischemia/infarction, anxiety, pain, fever, CNS tumor
Lung/Airway: Pulmonary embolism, restrictive lung disease, bronchospasm, pneumonia due
to hypoxic drive
Renal Compensation for respiratory alkalosis:
Acute respiratory alkalosis: for every pCO2 decrease by 10, HCO3 decrease by 2
Chronic respiratory alkalosis: for every pCO2 decrease by 10, HCO3 decrease by 5
Note: Respiratory alkalosis is the only acid-base disturbance where pH can return to normal
Both sepsis and salicylate O/D cause both anion gap metabolic acidosis and respiratory alkalosis
24.
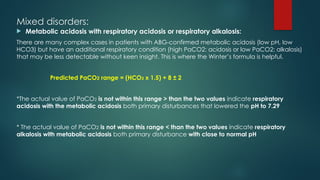
Mixed disorders:
Metabolicacidosis with respiratory acidosis or respiratory alkalosis:
There are many complex cases in patients with ABG-confirmed metabolic acidosis (low pH, low
HCO3) but have an additional respiratory condition (high PaCO2: acidosis or low PaCO2: alkalosis)
that may be less detectable without keen insight. This is where the Winter’s formula is helpful.
Predicted PaCO2 range = (HCO3 x 1.5) + 8 ± 2
*The actual value of PaCO2 is not within this range > than the two values indicate respiratory
acidosis with the metabolic acidosis both primary disturbances that lowered the pH to 7.29
* The actual value of PaCO2 is not within this range < than the two values indicate respiratory
alkalosis with metabolic acidosis both primary disturbance with close to normal pH
Delta Ratio: Isto determine concomitant or mix disorders with
elevated anion gap metabolic acidosis( AGMA) and or
NAGMA( non- anion gap acidosis)
Delta Ratio = measured AG- normal AG(12) / normal HCO3-(24) – measured HCO3-
If the :
delta ratio is <1 then is pure AGMA
delta ratio is 1-2 then is AGMA with NAGMA
delta ration >2 then is AGMA with Metabolic alkalosis
Clinical Vignette:
35yearold female presents to the ER with headache, altered sensorium
and muscle weakness. A history of using sliming tea. Serum electrolyte and
ABG are as follows:
pH: 7.48( 7.35-7.45)
PaCo2: 47 ( 35-45)mm Hg
HCO-3: 38 mmol/l ( 24-32)
PaO2 : 95 ( 75-100) mm Hg
Which of the following diagnosis is the most appropriate?
A. Metabolic acidosis without respiratory compensation
B. Metabolic alkalosis with respiratory compensation
C. Respiratory acidosis without renal compensation
D. Respiratory alkalosis with renal compensation
31.
Clinical Vignette:
A15year old male present to the ER unconscious. Glasgow scale 11, RR 20cpm, PR
120bpm. Blood chemistry results as follows:
sodium: 130mmol/l( 135-145) PaCO2: 38 mmHg( 35-45)
potassium: 10 mmol/l ( 3.5-5.0) Pa O2: 95 mmHg( 75-100)
chloride: 92mmol/l ( 95-105) Urine positive for ketones
bicarbonate: 10 mmol/l ( 24-32)
glucose: 35mmol/l ( 5.5-11.1)
pH 7.10 ( 7.35-7.45)
Which of the differential diagnosis is false?
A. Respiratory acidosis
B. Diabetic ketoacidosis
C. Hyperkalemia
D. Hyponatremia
32.
Clinical Vignette:
Thefollowing ABG for a patient with a history of poorly controlled diabetes and recent
diagnosis of diabetic ketoacidosis (DKA). DKA is commonly associated with an ABG-
confirmed metabolic acidosis:
pH= 7.29( 7.35-7.45)
PaCO2=38 mmHg( 35-45)mm Hg
HCO3=17 mEq/L ( 24-32)
Predict the acid-base disturbance?
Ans: used the winter’s formula to predict any mixed disorder?
Predicted PaCO2 = (HCO3 x 1.5) + 8 ± 2 = 31.5 to 35.5, the actual value of PaCO2=38 mmHg
*The actual value of PaCO2 is not within this range and > than the two values which indicate
respiratory acidosis with the metabolic acidosis both primary disturbances that lowered the
pH to 7.29
33.
References:
Guyton andHall, Textbook of Medical Physiology 14th
edition, Elsevier Publishers. Chpt 31, pp403-420
Respiratory Physiology by John B. West 10th
edition ,Wolters Kluwer Publishers. Chpt 6, pp96-103
Physiology by Costanza. 5th
edition, Elsevier Publishers. Chpt 7, pp 303-327
NEF @ 2007 nursing educational consultant, inc. derived caricatures



![Introduction:
pH= -log10 [H+]
[H+] ions are precisely regulated by the body at 37–43 neq/L with arterial blood having a normal pH range of 7.35
to 7.45(7.4+ 0.05), abnormal pH leads to physiological and biochemical changes with sometimes fatal
consequences.
Major ICF ( intra cellular fluid) buffers:
Proteins : Important intracellular buffers Hemoglobin
H+ + HbO2 HHb + O2
Organic phosphates (ATP, AMP, ADP)
(60–70% of buffering occurs inside cells)
Major ECF( extra cellular fluid) buffers:
Bicarbonate : Is the most important ECF buffer in blood plasma
* H2O + CO2 H2CO3 H+
+ HCO3
−
Phosphate-biphosphate : Is important renal tubular buffering
HPO4− + H+ H2PO4 −
Ammonia : Also, important renal tubular buffering
NH3 + H+ NH4 +](https://image.slidesharecdn.com/acidbasedisturbances-250523194803-9f3a6cb5/85/Acid-Base-Disturbances-and-pathological-conditions-3-320.jpg)
![ Henderson – Hasselbalch Equation
pH = -log [H+] ~ 6.1( pKa) + log [HCO3-] / (0.03)(pCO2) pKa = 6.1
Titration Curve for Bicarbonate Buffer System
The carbon-dioxide/bicarbonate buffer is the most important buffer in extracellular fluid even though the
concentration of the components are low and pKa of the system is 6.1, which is not very close to normal
extracellular fluid pH (7.4).
Reason: To maintain a pH 7.4 the components of the system
(CO2 and HCO3−) are closely regulated by the lungs and the
Kidneys, respectively.](https://image.slidesharecdn.com/acidbasedisturbances-250523194803-9f3a6cb5/85/Acid-Base-Disturbances-and-pathological-conditions-4-320.jpg)
![Determine acid - base disorders:
CO2 + H2O *carbonic anhydrase H2CO3 H+ + HCO3- *pH= [HCO3-] / (pCO2)
Step 1: Look at the pH to determine acidotic or alkalotic condition
Step 2: Look at the levels of PaCO2 and HCO3 to determine primary disorder
If the change in HCO3 is consistent with change in pH ,then it is a metabolic disorder
If the change in Pa CO2 is consistent with change in pH, then it is a respiratory disorder
Step 3: look to see if there is another primary disorder](https://image.slidesharecdn.com/acidbasedisturbances-250523194803-9f3a6cb5/85/Acid-Base-Disturbances-and-pathological-conditions-8-320.jpg)
![Summary classification of Acid-Base Disturbances:
CO2 + H2O *carbonic anhydrase H2CO3 H+ + HCO3- pH= [HCO3-] /
(pCO2)](https://image.slidesharecdn.com/acidbasedisturbances-250523194803-9f3a6cb5/85/Acid-Base-Disturbances-and-pathological-conditions-13-320.jpg)