Applications of ABG
•To document respiratory failure and assessing its severity
• To monitor patients on mechanical ventilation and assist in weaning
• Identification and monitoring of acid base disorders
• Assessment of the responses to therapeutic interventions
• Abnormal Hb(metHb, SulfHb)
3.
Contraindications for ABGsampling
• Abnormal modified Allen’s test.
• Local infection, thrombosis at the puncture site
• Distorted anatomy at the puncture site.( AV fistula, aneurysm and
congenital and acquired vascular malformations)
• Severe peripheral vascular disease of the artery selected for sampling.
• Active Raynaud’s syndrome
4.
Obtaining an ABG
•ABG is commonly obtained by percutaneous needle puncture.
• Sites- 1) Radial artery – Preferred site (Easily accessible, collateral flow
present, superficial)
2) Femoral artery
3) Brachial artery To be used in case of emergencies.
4) Dorsalis pedis artery
• Collateral circulation must be ensured- Modified Allen’s test.
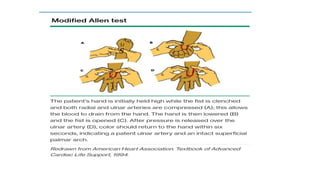
Modified Allen’s Test
•It is done to test the patency of ulnar artery( collateral circulation) so
that we can puncture the radial artery for abg analysis.
8.
Complications
Common
• Local painand paresthesia
• Bruising and hematoma
Less common
• Infection at puncture site
• Arterial occlusion
• Air/Thrombus embolism
• Pseudoaneurysm formation
• Vasovagal response
• Persistent pain/paresthesia
9.
Preanalytical errors
• Delayedanalysis
PaCO2 increases @ 3-10 mm/ hour and PaO2 decreases.
• Excessive heparin
1) 0.05ml of heparin is required per mL of blood.
2)Dilutional effect occurs with larger volume of heparin resulting in
decreased bicarbonate and PaCO2.
3)Risk is increased with increased size of needle and decreased volume of
sample.
10.
Preanalytical errors
• Airbubbles
1) pO2 150mm Hg and pCO2 0mm Hg ( in air bubble)
2) Spuriously p02 and pCO2
3) Prevention- Seal syringe immediately after sampling.
• WBC count(Spurious hypoxemia)
1)0.1 ml O2 consumed/dL in 10 minutes in patients with Normal TLC
2) Markedly increased consumption in patients with very high TLC
3) Prevention- Chilling and immediate analysis.
Hypoxia vs Hypoxemia
•Hypoxia refers to decreased levels of tissue oxygenation
• Hypoxemia is a reduction in the arterial oxygen tension.
• SaO2- Direct measurement of percentage of oxyhemoglobin in blood ( cal
• PaO2(arterial oxygen tension) - Amount of oxygen dissolved in plasma.
PaO2 of 80 – 105 mmHg on room air - normal.
PO2 of < 80 mmHg on room air - hypoxemia.
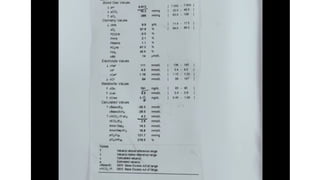
Validity of ABG
•Validity of ABG-
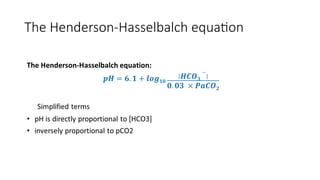
• Derivation using the Henderson-Hasselbalch
equation:
• [H+] = 24(PaCO2)/[HCO3-]
• If measured and calculated [H+] inconsistent
Invalid ABG
20.
ACIDOSIS AND ALKALOSIS
•ACIDOSIS : pH = <7.35
• When HCO3 is low, it is metabolic acidosis
• When pCO2 is high, it is respiratory acidosis
• ALKALOSIS : pH = > 7.45
• When HCO3 is high, it is metabolic alkalosis
• When pCO2 is low, it is respiratory alkalosis
21.
Respiratory and metabolic
•Respiratory – Primary alteration in ventilation and resultant excessive elimination
or retention of CO2
• Metabolic – Primary process in any organ system other than lung (GIT, Kidneys)
22.
Compensation
• The normalresponse of the respiratory system or kidneys to change in pH
induced by a primary acid-base disorder. In 1⁰respiratory disorder kidney is
responsible for compensation and vice versa
• Compensatory response depends on proper functioning of organ system (lungs or
kidney)
• Respiratory compensation occurs rapidly within minutes to hours(starts within 30
minutes and is complete within 12- 24hrs)
• Metabolic compensation starts within hours and complete within 3-5days
• Overcompensation never occurs
ZZ ZZZZ
23.
Acute or chronic
•In respiratory disorders acuteness or chronicity can be assessed by
1)History
2)H+/PaCO2 ratio
<0.3 chronic
>0.8 acute
0.3-0.8 Acute on chronic
24.
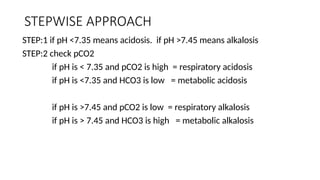
STEPWISE APPROACH
STEP:1 ifpH <7.35 means acidosis. if pH >7.45 means alkalosis
STEP:2 check pCO2
if pH is < 7.35 and pCO2 is high = respiratory acidosis
if pH is <7.35 and HCO3 is low = metabolic acidosis
if pH is >7.45 and pCO2 is low = respiratory alkalosis
if pH is > 7.45 and HCO3 is high = metabolic alkalosis
25.
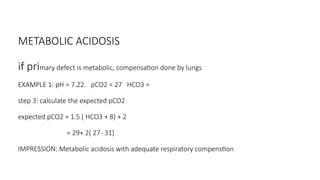
METABOLIC ACIDOSIS
if primarydefect is metabolic, compensation done by lungs
EXAMPLE 1: pH = 7.22. pCO2 = 27 HCO3 =
step 3: calculate the expected pCO2
expected pCO2 = 1.5 ( HCO3 + 8) + 2
= 29+ 2( 27- 31)
IMPRESSION: Metabolic acidosis with adequate respiratory compenstion
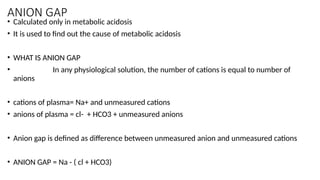
ANION GAP
• Calculatedonly in metabolic acidosis
• It is used to find out the cause of metabolic acidosis
• WHAT IS ANION GAP
• In any physiological solution, the number of cations is equal to number of
anions
• cations of plasma= Na+ and unmeasured cations
• anions of plasma = cl- + HCO3 + unmeasured anions
• Anion gap is defined as difference between unmeasured anion and unmeasured cations
• ANION GAP = Na - ( cl + HCO3)
28.
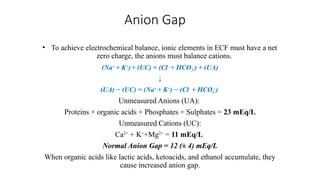
Anion Gap
• Toachieve electrochemical balance, ionic elements in ECF must have a net
zero charge, the anions must balance cations.
(Na+
+ K+
)+ (UC) = (Cl-
+ HCO3
-
) + (UA)
↓
(UA) − (UC) = (Na+
+ K+
) − (Cl-
+ HCO3
-
)
Unmeasured Anions (UA):
Proteins + organic acids + Phosphates + Sulphates = 23 mEq/L
Unmeasured Cations (UC):
Ca2+
+ K+
+Mg2+
= 11 mEq/L
Normal Anion Gap = 12 (± 4) mEq/L
When organic acids like lactic acids, ketoacids, and ethanol accumulate, they
cause increased anion gap.
29.
CAUSES OF METABOLICACIDOSIS
• DECREASED HCO3
• Increased utilization of HCO3
• Increased excretion of HCO3
• INCREASED UTILIZATION OF HCO3
• CAUSES:
• Whenever excess acid builds up in the body,
• H* + HCO3 = H2CO3 + Unmeasured anion
• lactic acid + HCO3 = H2CO3 + lactate anion forms
30.
• ANION GAP
•Unmeasured anion - Unmeasured cation
• SO, in case of excess acid in the body, the unmeasured anion increases
31.
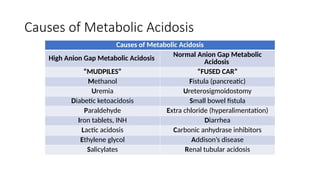
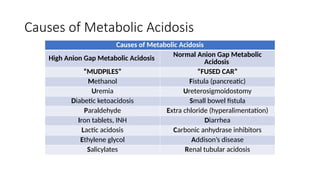
Causes of MetabolicAcidosis
Causes of Metabolic Acidosis
High Anion Gap Metabolic Acidosis Normal Anion Gap Metabolic
Acidosis
“MUDPILES” “FUSED CAR”
Methanol Fistula (pancreatic)
Uremia Ureterosigmoidostomy
Diabetic ketoacidosis Small bowel fistula
Paraldehyde Extra chloride (hyperalimentation)
Iron tablets, INH Diarrhea
Lactic acidosis Carbonic anhydrase inhibitors
Ethylene glycol Addison’s disease
Salicylates Renal tubular acidosis
32.
INCREASED LOSS OFHCO3
• loss occurs through either git or renal
• in either cases, body reclines cl- , so they are called hyperchloremic metabolic acidosis
•
• WHAT WILL HAPPEN TO ANION GAP?
• Na - ( cl + HCO3)
• cl increases and HCO3 decreases, so there will be a normal anion gap.
33.
Causes of MetabolicAcidosis
Causes of Metabolic Acidosis
High Anion Gap Metabolic Acidosis Normal Anion Gap Metabolic
Acidosis
“MUDPILES” “FUSED CAR”
Methanol Fistula (pancreatic)
Uremia Ureterosigmoidostomy
Diabetic ketoacidosis Small bowel fistula
Paraldehyde Extra chloride (hyperalimentation)
Iron tablets, INH Diarrhea
Lactic acidosis Carbonic anhydrase inhibitors
Ethylene glycol Addison’s disease
Salicylates Renal tubular acidosis
34.
URINARY ANION GAP
•How to find the loss of bicarbonate is through git or renal?
• found by calculating urinary anion gap
• URINARY ANION GAP
• Sum of cations in urine = sum of anions in urine
• Na* + k* + umc = cl + uma ( HCO3 in urine is nil)
• If urinary anion gap is negative, cause is git
• If urinary anion gap is positive, cause is renal
35.
TAKE HOME MSGFOR METABOLIC ACIDOSIS
• METABOLIC ACIDOSIS
• EXPECTED PCO2
• ANION GAP - To find out the cause of metabolic acidosis
• If Anion gap in increased = due to excess acid in the body
• if anion gap is normal = either due to git or renal
• git or renal is found by Urinary anion gap
36.
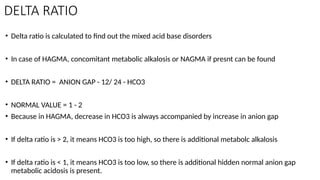
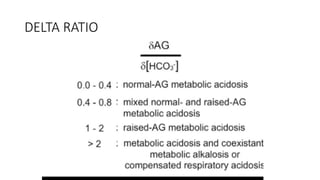
DELTA RATIO
• Deltaratio is calculated to find out the mixed acid base disorders
• In case of HAGMA, concomitant metabolic alkalosis or NAGMA if presnt can be found
• DELTA RATIO = ANION GAP - 12/ 24 - HCO3
• NORMAL VALUE = 1 - 2
• Because in HAGMA, decrease in HCO3 is always accompanied by increase in anion gap
• If delta ratio is > 2, it means HCO3 is too high, so there is additional metabolc alkalosis
• If delta ratio is < 1, it means HCO3 is too low, so there is additional hidden normal anion gap
metabolic acidosis is present.
RESPIRATORY ACIDOSIS
• Incase of primary respiratory disorder, the compensation is done by kidneys
• ACUTE. for every 10 mm increase in pCO2, HCO3 will increase by 1
• CHRONIC for every 10 mm increase in pCO2, HCO3 will increase by 3.5
• EXAMPLE 1 : pH =7.34. pCO2 = 60. HCO3 = 32
• acidosis
• respiratory acidosis
• here pCO2 increased by 20 and HCO3 by 4
• IMPRESSION : Chronic respiratory acidosis with metabolic compensation
RESPIRATORY ALKALOSIS
In ACUTE= if there is 10 mm decrease in pCO2, HCO3 decrease by 2
In CHRONIC = if there is 10 mm decrease in pCO2, HCO3 decrease by 5
EXAMPLE 1 : pH = 7.5. pCO2 = 25. HCO3 = 20
* alkalosis
* respiratory alkalosis
*15 mm decrease by pCO2, HCO3 decrease by 2
*IMPRESSION: acute respiratory alkalosis with adequate metabolic compensation
EXAMPLE 2 : pH = 7.5. pCO2 = 30. HCO3 = 29
*respiratory alkalosis
* respiratory alkalosis with metabolic alkalosis
42.
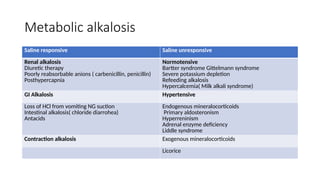
Metabolic alkalosis
Saline responsiveSaline unresponsive
Renal alkalosis
Diuretic therapy
Poorly reabsorbable anions ( carbenicillin, penicillin)
Posthypercapnia
Normotensive
Bartter syndrome Gittelmann syndrome
Severe potassium depletion
Refeeding alkalosis
Hypercalcemia( Milk alkali syndrome)
GI Alkalosis Hypertensive
Loss of HCl from vomiting NG suction
Intestinal alkalosis( chloride diarrohea)
Antacids
Endogenous mineralocorticoids
Primary aldosteronism
Hyperreninism
Adrenal enzyme deficiency
Liddle syndrome
Contraction alkalosis Exogenous mineralocorticoids
Licorice
43.
Respiratory alkalosis
• pH>7.45pCO2<35 mm Hg
• Causes- 1) CNS stimulation – pain, anxiety, fever, CVA, Meningoencephalitis,
Tumor, Trauma
2) Hypoxemia/ Tissue hypoxia- High altitude, pneumonia, severe Anemia
3)Drugs-
4) Heat exposure, hepatic failure, recovery from metabolic acidosis
44.
• 92 yrsMALE, K/C/O COPD, CAME WITH COMPLAINTS
• SOB (GRADE 3-4) FOR 1wk
• COUGH WITH EXPECTORATION FOR 1 wk
• ORTHOPNEA +
• H/O FEVER FOR 1wk
• H/O DECREASED URINE OUTPUT FOR 1 day
• RS- BAE+ AND B/L WHEEZE + AND B/L CREPTS +
46.
• A 45YRS MALE CAME TO ER WITH COMPLAINTS OF
• ABDOMINAL DISCOMFORT FOR 1 DAY
• H/O BLOOD VOMITING 2 EPISODES SINCE ONE HOUR
• H/O BLACK COLOURED STOOL SINCE 3 DAYS
• H/O SOB ON EXERTION SINCE 3 DAYS
• PT DROWSY, P/A EXAMINATION = SOFT, DIFFUSE TENDERNESS +
48.
A 59 OLDFEMALE CAME TO ER WITH C/O
GENERALIZED SWELLING, GRADUALLY INCREASED SINCE 2 DAYS
H/O ITCHING AND REDNESS ALL OVER THE BODY SINCE 15 days
H/O SOB ON EXERTION + SINCE 2 DAYS
H/O DECREASED URINE OUTPUT FOR 4 days
H/O LOSS OF APPETITE +
RS - BAE+ B/L BASAL CREPTS +
50.
• A 74YR OLD FEMALE PRESENTED TO ER WITH C/O
• DECREASED APPETITE FOR 3 DAYS
• INCREASED SOB SINCE MORNING
• ALTERED SENSORIUM SINCE ONE HOUR
• H/O VOMOTING , 2 EPISODES SINCE MRNG
• AIRWAY - THREATENED CNS= E3 V1 M5 ALTERED SENSORIUM
• CVS = BP - NR PR - 66/MIN
• RS - BAE+ NO ADDED SOUNDS
52.
Summary
• ABG issimple investigation
• Do interpretation in protocolized way

![Validity of ABG
• Validity of ABG-
• Derivation using the Henderson-Hasselbalch
equation:
• [H+] = 24(PaCO2)/[HCO3-]
• If measured and calculated [H+] inconsistent
Invalid ABG](https://image.slidesharecdn.com/abginterpretation-250213115803-808cd2c4/85/Acid-Base-Gas-analysis-clinical-interpretation-19-320.jpg)