CONJUNCTIVAL TUMOURS
PRESENTER –Dr AARUSHI (1st
year resident)
MODERATOR – Dr URMILA KUMARI
DHIR HOSPITAL AND POST GRADUATE
INSTITUTE OF OPHTHALMOLOGY
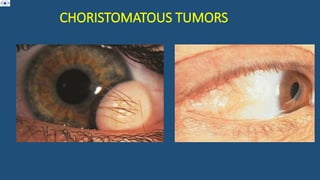
3.
CONJUNCTIVAL CYST
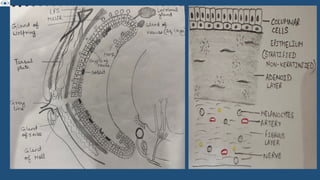
• Thinwalled , benign cystic lesions lined with
non keratinizing epithelium containing serous
fluid
• S/S : asymptomatic, cosmetic disfigurement,
reduced motility, FB sensation , dry eye d/t
unstable tear film , proptosis , BOV
• Inclusion cysts constitute 80% of all cystic
lesions of conjunctiva
• Average age : 47 yrs , M=F
4.
• Risk factors:
• Inflammatory conditions : pterygium ,
pingecula
• chronic keratoconjunctivitis
• Trauma , surgery
• Sub tenon anesthesia
• Pathophysiology :
• Inclusion of conj epithelium into substantia propria
• May contain gas , fluid , semisolid material with membranous framework
5.
• 1. PrimaryInclusion Cysts:
• Congenital:
• Present at birth d/t excessive conjunctival invagination during embryonic
period
• Acquired:
• Develop d/t chronic inflammation where loose ep gets implanted into deeper
tissue, even with minor trauma
• 2. Secondary Inclusion Cysts:
• Trauma or surgery such as strabismus surgery
• Inflammation : pterygium , pingueculitis, chronic keratoconjunctivitis
• 3. Infective cysts :
• Seen in hydatid disease , cysticercosis
6.
Treatment :
• Observation/ intervention depends on size , patient comfort
• Definitive treatment : excision
• Others : aspiration on slit lamp 27-30G needle under TA
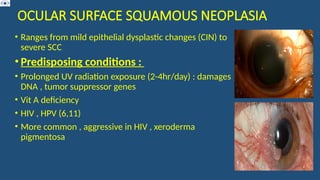
OCULAR SURFACE SQUAMOUSNEOPLASIA
• Ranges from mild epithelial dysplastic changes (CIN) to
severe SCC
• Predisposing conditions :
• Prolonged UV radiation exposure (2-4hr/day) : damages
DNA , tumor suppressor genes
• Vit A deficiency
• HIV , HPV (6,11)
• More common , aggressive in HIV , xeroderma
pigmentosa
10.
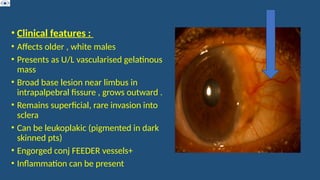
• Clinical features:
• Affects older , white males
• Presents as U/L vascularised gelatinous
mass
• Broad base lesion near limbus in
intrapalpebral fissure , grows outward .
• Remains superficial, rare invasion into
sclera
• Can be leukoplakic (pigmented in dark
skinned pts)
• Engorged conj FEEDER vessels+
• Inflammation can be present
11.
MORPHOLOGICAL FORMS
• 1)gelatinous mass with superficial vessels : most
common
• 2) Nodular : propensity for rapid growth
• 3) Diffuse : can masquerade as membranous /
chronic Conjunctivitis (no papillary , follicular rxn )
12.
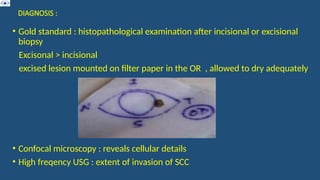
DIAGNOSIS :
• Goldstandard : histopathological examination after incisional or excisional
biopsy
Excisonal > incisional
excised lesion mounted on filter paper in the OR , allowed to dry adequately
• Confocal microscopy : reveals cellular details
• High freqency USG : extent of invasion of SCC
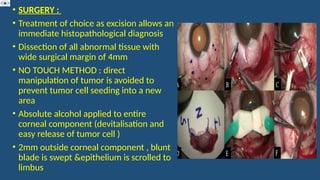
• SURGERY :
•Treatment of choice as excision allows an
immediate histopathological diagnosis
• Dissection of all abnormal tissue with
wide surgical margin of 4mm
• NO TOUCH METHOD : direct
manipulation of tumor is avoided to
prevent tumor cell seeding into a new
area
• Absolute alcohol applied to entire
corneal component (devitalisation and
easy release of tumor cell )
• 2mm outside corneal component , blunt
blade is swept &epithelium is scrolled to
limbus
17.
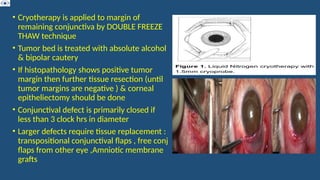
• Cryotherapy isapplied to margin of
remaining conjunctiva by DOUBLE FREEZE
THAW technique
• Tumor bed is treated with absolute alcohol
& bipolar cautery
• If histopathology shows positive tumor
margin then further tissue resection (until
tumor margins are negative ) & corneal
epitheliectomy should be done
• Conjunctival defect is primarily closed if
less than 3 clock hrs in diameter
• Larger defects require tissue replacement :
transpositional conjunctival flaps , free conj
flaps from other eye ,Amniotic membrane
grafts
18.
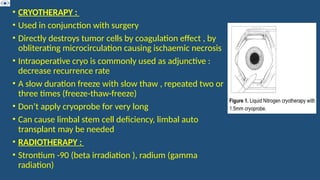
• CRYOTHERAPY :
•Used in conjunction with surgery
• Directly destroys tumor cells by coagulation effect , by
obliterating microcirculation causing ischaemic necrosis
• Intraoperative cryo is commonly used as adjunctive :
decrease recurrence rate
• A slow duration freeze with slow thaw , repeated two or
three times (freeze-thaw-freeze)
• Don’t apply cryoprobe for very long
• Can cause limbal stem cell deficiency, limbal auto
transplant may be needed
• RADIOTHERAPY :
• Strontium -90 (beta irradiation ), radium (gamma
radiation)
19.
• TOPICAL CHEMOTHERAPY: MITOMYCIN –C
• Anti-tumor antibiotic , Inhibits DNA synthesis
• It leads to generation of alkylating agents , redox cycling
that produce active oxygen species leading to DNA
damage
• Produces cell death by apoptosis , necrosis
• QID with 1 week on and 2-3 week break = 1 cycle
• The on & off regimen prevents damage to more slowly
dividing epithelial cells & limbal stem cells , allowing
them to repair their DNA
• If not given break , may lead to : corneal epitheliopathy ,
scleral ulceration , uveitis , cataract , punctal stenosis
20.
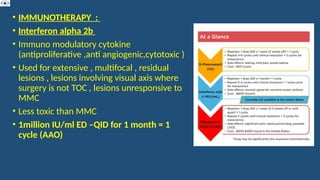
• IMMUNOTHERAPY :
•Interferon alpha 2b
• Immuno modulatory cytokine
(antiproliferative ,anti angiogenic,cytotoxic )
• Used for extensive , multifocal , residual
lesions , lesions involving visual axis where
surgery is not TOC , lesions unresponsive to
MMC
• Less toxic than MMC
• 1million IU/ml ED –QID for 1 month = 1
cycle (AAO)
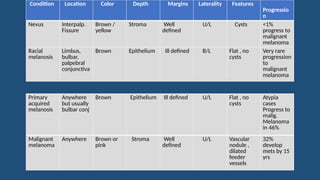
Condition Location ColorDepth Margins Laterality Features
Progressio
n
Nevus Interpalp.
Fissure
Brown /
yellow
Stroma Well
defined
U/L Cysts <1%
progress to
malignant
melanoma
Racial
melanosis
Limbus,
bulbar,
palpebral
conjunctiva
Brown Epithelium Ill defined B/L Flat , no
cysts
Very rare
progression
to
malignant
melanoma
Primary
acquired
melanosis
Anywhere
but usually
bulbar conj
Brown Epithelium Ill defined U/L Flat , no
cysts
Atypia
cases
Progress to
malig.
Melanoma
in 46%
Malignant
melanoma
Anywhere Brown or
pink
Stroma Well
defined
U/L Vascular
nodule ,
dilated
feeder
vessels
32%
develop
mets by 15
yrs
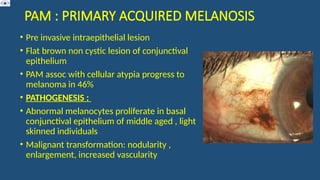
PAM : PRIMARYACQUIRED MELANOSIS
• Pre invasive intraepithelial lesion
• Flat brown non cystic lesion of conjunctival
epithelium
• PAM assoc with cellular atypia progress to
melanoma in 46%
• PATHOGENESIS :
• Abnormal melanocytes proliferate in basal
conjunctival epithelium of middle aged , light
skinned individuals
• Malignant transformation: nodularity ,
enlargement, increased vascularity
25.
• MANAGEMENT :
•Excisional biopsy
• All palpebral pigmented lesions should be excised
• Lesions that show atypia : adjunctive cryotherapy , MMC
• Small PAM (1–2 clock hours): Observe with yearly follow-up unless changes like
nodularity, thickening, or vascularity occur, then excision is needed.
• Moderate-sized PAM (2–5 clock hours): Requires excision with cryotherapy to
margins.
• Large PAM (>5–6 clock hours): Suspicious areas should be excised, and a map
biopsy of all quadrants (even those appearing normal) is recommended.
26.
• Primary Treatment:Excision with 4–5 mm tumor-free margins plus
double-freeze, slow-thaw cryotherapy to conjunctival edges is the
standard approach.
• Corneal Involvement: If pigmentation extends onto the cornea, apply
absolute alcohol for 1 minute followed by epitheliectomy.
• Topical Chemotherapy: Mitomycin C (0.02–0.04%) is used postoperatively
in cycles (1 week treatment, 1–2 week break), with punctal plugs
• Treatment Duration: Typically requires 2–3 cycles until pigmentation
resolves.
27.
MALIGNANT MELANOMA
• Mcarises from PAM or can exist from nevus or de novo
• Median age : 62 years
• Pigmented or tan , elevated lesion on limbal /bulbar
/forniceal/palpebral conjunctiva
• Prominent feeder vessels present , Highly vascularised , bleed easily
• MC on bulbar conj / limbus
• Outcome : bulbar melanomas have better prognosis than those on
palpebral conj , fornix or caruncle
• Local recurrence , distant mets , multiple recurrences (can invade
globe/orbit)
• Intralymphatic spread increase risk of mets
• R/F for mets : large size , multicentric , epitheliod cell type ,
lymphatic invasion
29.
MANAGEMENT
• Excisional biopsy: Excision of conj 4mm beyond clinically apparent margins
• Excision of thin lamellar scleral flap beneath tumor
• Treat remaining sclera with absolute alcohol
• Double freeze thaw Cryotherapy to conjunctival margins
• Primary closure or conj / AMG
• Topical mitomycin-C for residual disease
• Orbital exenteration- advanced disease or palliative treatment
• Poor prognostic factors :
• Melanomas arising denovo , tumors not involving limbus(extralimbal) ,
residual involvement at surgical margins
30.
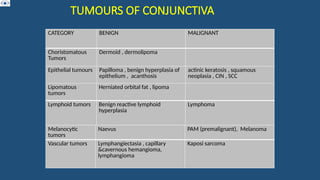
CONJUNCTIVAL LYMPHOMA
• Monoclonalproliferation of lymphocytes
(nodal,extranodal)
• Ocular adenexal lymphomas are typically of
B cell origin
• Pathological Types : Extranodal marginal
zone lymphoma ( ENMZL) , Follicular
lymphoma (FL) , Mantle cell lymphoma
(MCL) , Diffuse large B cell lymphoma
(DLBCL)
• Predisposing factors :
• Immune deficiency , autoimmune
conditions , infections (H.pylori ,
chalamydia psittaci ) , genetic mutations
31.
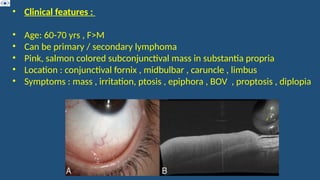
• Clinical features:
• Age: 60-70 yrs , F>M
• Can be primary / secondary lymphoma
• Pink, salmon colored subconjunctival mass in substantia propria
• Location : conjunctival fornix , midbulbar , caruncle , limbus
• Symptoms : mass , irritation, ptosis , epiphora , BOV , proptosis , diplopia
32.
• Management :
•Depends on extent of periocular & systemic involvement , general
health
• 1) Only conjunctival lymphoma (no systemic inv) : complete surgical
resection , External beam radiotherapy , rituximab
• 2) Periocular/systemic inv present : systemic rituximab , chemotherapy,
immunotherapy
• Prognosis :
• 5yr survival 97% ENMZL , 82% for FL , 55% DLBCL , 9% MCL






































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


