Schoen Bendingthecurve Exhibits Ppt
•Download as PPT, PDF•
0 likes•268 views

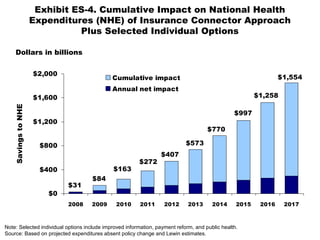
This document summarizes the projected cumulative impact on national health expenditures from 2008 to 2017 of an insurance connector approach combined with selected individual options like improved information, payment reform, and public health initiatives. It shows that this combination is estimated to reduce cumulative NHE by $1.554 trillion by 2017, with an annual net impact ranging from $84 billion in savings in 2008 to $272 billion in savings in 2017.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Schoen Bendingthecurve Exhibits Ppt
Similar to Schoen Bendingthecurve Exhibits Ppt (20)
More from Brian Ahier
More from Brian Ahier (20)
Recently uploaded
Recently uploaded (20)
Schoen Bendingthecurve Exhibits Ppt
- 1. Exhibit ES-4. Cumulative Impact on National Health Expenditures (NHE) of Insurance Connector Approach Plus Selected Individual Options $31 $1,554 $1,258 $997 $770 $573 $407 $84 $163 $272 $0 $400 $800 $1,200 $1,600 $2,000 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 Cumulative impact Annual net impact Dollars in billions Note: Selected individual options include improved information, payment reform, and public health. Source: Based on projected expenditures absent policy change and Lewin estimates. SavingstoNHE
- 2. Exhibit ES-5. Total National Health Expenditures, 2008–2017 Projected and Various Scenarios 3.0 3.2 3.4 3.6 3.9 4.1 4.4 2.3 2.8 2.6 2.4 2.9 3.0 3.2 3.4 3.7 3.9 4.1 2.7 3.6 3.4 3.3 3.1 3.0 2.8 2.6 2.5 2.4 2.9 $2.0 $2.5 $3.0 $3.5 $4.0 $4.5 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 Projected under current system Insurance Connector plus selected individual options* Spending at current proportion (16.2%) of GDP * Selected individual options include improved information, payment reform, and public health. Source: Based on projected expenditures absent policy change and Lewin estimates. Dollars in trillions
- 3. Exhibit 1. Projected National Health Expenditures (NHE) by Payer Source, 2005–2016 * Consumer payments include out-of-pocket payments and private health insurance. Source: J. A. Poisal, C. Truffer, S. Smith et al., “Health Spending Projections Through 2016: Modest Changes Obscure Part D’s Impact,” Health Affairs Web Exclusive (Feb. 21, 2007):w242–w253. Projected Total 2005 2011 2016 NHE (in billions) $1,987.7 $2,966.4 $4,136.9 NHE as percent of GDP 16.0% 17.5% 19.6% Payer Source Private $1,085.0 $1,566.1 $2,123.3 Consumer Payments* 943.8 1,347.0 1,811.9 Other Private Funds 141.2 219.1 311.4 Public 902.7 1,400.3 2,013.6 Federal 643.7 1027.4 1,486.5 State and Local 259.0 372.9 527.1
- 4. Exhibit 2. International Comparison of Health Spending, 1980–2005 0 1000 2000 3000 4000 5000 6000 7000 1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 United States Germany Canada France Australia United Kingdom 0 2 4 6 8 10 12 14 16 1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 United States Germany Canada France Australia United Kingdom Source: OECD Health Data 2007. Average spending on health per capita ($US PPP) Total health expenditures as percent of GDP
- 5. Exhibit 3. Financial Burden for Low- and Middle-Income Families Is Increasing 26 24 16 7 33 24 23 10 0 25 50 <100% FPL 100% to <200% FPL 200% to <400% FPL 400%+ FPL 1996 2003 Percent of nonelderly adults spending 10% or more of disposable income on family out-of-pocket medical costs and premiums Note: Financial burden includes out-of-pocket costs for premiums for private insurance and other health services. Source: J. S. Banthin and D. M. Bernard, “Changes in Financial Burdens for Health Care: National Estimates for the Population Younger than 65 Years,” Journal of the American Medical Association, Dec. 13, 2006 296(22):2712–19.
- 6. Exhibit 4. One-Third of Adults Ages 19–64 Are Uninsured or Underinsured, as Are Two-Thirds of Low-Income Adults 65 83 32 19 4 9 26 49 13 0% 20% 40% 60% 80% 100% Total 200% of poverty or more Under 200% of poverty Uninsured during year Underinsured* Insured, not underinsured * Underinsured defined as insured all year but experienced one of the following: medical expenses equaled 10% or more of income; medical expenses equaled 5% or more of incomes if low-income (<200% of poverty); or deductibles equaled 5% or more of income. Data: 2003 Commonwealth Fund Biennial Health Insurance Survey (Schoen et al. 2005b). Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2006. Percent
- 7. Exhibit 5. Growth in National Health Expenditures (NHE) Under Various Scenarios Source: The Commonwealth Fund; data from J. A. Poisal, C. Truffer, S. Smith et al., “Health Spending Projections Through 2016: Modest Changes Obscure Part D’s Impact,” Health Affairs Web Exclusive (Feb. 21, 2007):w242–w253. NHE, in trillions of dollars 7 1.75 2.00 2.25 2.50 2.75 3.00 3.25 3.50 3.75 4.00 4.25 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 Baseline NHE One-time savings scenario Slowing trend scenario Reduced level & trend scenario $1.99 T in 2005 Cumulative savings projections to 2016: One-time savings of 5%: $1.56 trillion Slowing trend by 1% annually: $1.72 trillion Combination of one-time savings and slowing trend: $3.19 trillion $4.14 T $3.93 T $3.77 T $3.58 T (19.6% GDP) (18.6% GDP) (17.8% GDP) (16.9% GDP)
- 8. Exhibit 8. Distribution of 10-Year Impact on Spending from Promoting Health Information Technology -$87.8 $0.2 -$19.3 -$27.2 -$41.4 -$100 -$80 -$60 -$40 -$20 $0 $20 $40 Systemwide Federal Gov't State and Local Gov't Private Payer Households Dollars in billions SAVINGSCOSTS Source: Based on estimates by The Lewin Group for The Commonwealth Fund, 2007.
- 9. Exhibit 9. Distribution of 10-Year Impact on Spending from Center for Medical Effectiveness and Health Care Decision-Making -$367.5 -$97.7 -$49.1 -$107.1-$113.6 -$400 -$300 -$200 -$100 $0 $100 $200 Systemwide Federal Gov't State and Local Gov't Private Payer Households Dollars in billions SAVINGSCOSTS Source: Based on estimates by The Lewin Group for The Commonwealth Fund, 2007.
- 10. Exhibit 10. Distribution of 10-Year Impact on Spending from Patient Shared Decision-Making -$9.2 -$7.6 -$0.4-$0.2 -$1.2 -$10 -$8 -$6 -$4 -$2 $0 $2 Systemwide Federal Gov't State and Local Gov't Private Payer Households Dollars in billions SAVINGSCOSTS Source: Based on estimates by The Lewin Group for The Commonwealth Fund, 2007.
- 11. -$190.5 -$68.2 -$48.9 -$38.5-$34.9 -$250 -$200 -$150 -$100 -$50 $0 $50 $100 Systemwide Federal Gov't State and Local Gov't Private Payer Households Exhibit 11. Distribution of 10-Year Impact on Spending from Reducing Tobacco Use Dollars in billions Source: Based on estimates by The Lewin Group for The Commonwealth Fund, 2007. SAVINGSCOSTS
- 12. -$282.6 -$72.5 -$101.2 -$57.2-$51.8 -$400 -$300 -$200 -$100 $0 $100 Systemwide Federal Gov't State and Local Gov't Private Payer Households Exhibit 12. Distribution of 10-Year Impact on Spending from Reducing Obesity Dollars in billions SAVINGSCOSTS Source: Based on estimates by The Lewin Group for The Commonwealth Fund, 2007.
- 13. Exhibit 13. Distribution of 10-Year Impact on Spending from Positive Incentives for Health -$19.0 -$11.5 -$4.5 -$5.2 $2.2 -$25 -$20 -$15 -$10 -$5 $0 $5 $10 Systemwide Federal Gov't State and Local Gov't Private Payer Households Dollars in billions Source: Based on estimates by The Lewin Group for The Commonwealth Fund, 2007. SAVINGSCOSTS
- 14. Exhibit 14. Distribution of 10-Year Impact on Spending from Hospital Pay-for-Performance -$34.0 -$4.1 -$1.7-$0.8 -$27.4 -$40 -$30 -$20 -$10 $0 $10 $20 Systemwide Federal Gov't State and Local Gov't Private Payer Households Source: Based on estimates by The Lewin Group for The Commonwealth Fund, 2007. Dollars in billions SAVINGSCOSTS
- 15. Exhibit 15. Distribution of 10-Year Impact on Spending from Episode-of-Care Payment -$229.2 -$377.4 $39.7 $90.1 $18.3 -$500 -$400 -$300 -$200 -$100 $0 $100 $200 Systemwide Federal Gov't State and Local Gov't Private Payer Households Source: Based on estimates by The Lewin Group for The Commonwealth Fund, 2007. Dollars in billions SAVINGSCOSTS
- 16. Exhibit 16. Distribution of 10-Year Impact on Spending from Strengthening Primary Care and Care Coordination -$9.1 -$193.5 -$156.9 -$4.1 -$23.4 -$250 -$200 -$150 -$100 -$50 $0 $50 $100 Systemwide Federal Gov't State and Local Gov't Private Payer Households Source: Based on estimates by The Lewin Group for The Commonwealth Fund, 2007. Dollars in billions SAVINGSCOSTS
- 17. Exhibit 17. Distribution of 10-Year Impact on Spending from Limit on Federal Tax Exemptions for Premium Contributions -$131.1 -$55.2 -$19.3 $129.7 -$186.2 -$250 -$200 -$150 -$100 -$50 $0 $50 $100 $150 $200 Systemwide Federal Gov't State and Local Gov't Private Payer Households Source: Based on estimates by The Lewin Group for The Commonwealth Fund, 2007. Dollars in billions SAVINGSCOSTS
- 18. Exhibit 18. Distribution of 10-Year Impact on Spending from Reset Benchmark Rates for Medicare Advantage Plans -$49.6 -$124.0 $0.0 $0.0 $74.4 -$150 -$100 -$50 $0 $50 $100 $150 $200 Systemwide Federal Gov't State and Local Gov't Private Payer Households Source: Based on estimates by The Lewin Group for The Commonwealth Fund, 2007. Dollars in billions SAVINGSCOSTS
- 19. Exhibit 19. Distribution of 10-Year Impact on Spending from Competitive Bidding -$104.2 -$282.5 $0.0 $0.0 $178.3 -$400 -$300 -$200 -$100 $0 $100 $200 Systemwide Federal Gov't State and Local Gov't Private Payer Households Source: Based on estimates by The Lewin Group for The Commonwealth Fund, 2007. Dollars in billions SAVINGSCOSTS
- 20. Exhibit 20. Distribution of 10-Year Impact on Spending from Negotiated Prescription Drug Prices -$43.4 $7.5 $17.1 $3.5 -$71.5 -$100 -$80 -$60 -$40 -$20 $0 $20 $40 Systemwide Federal Gov't State and Local Gov't Private Employer Households Source: Based on estimates by The Lewin Group for The Commonwealth Fund, 2007. Dollars in billions SAVINGSCOSTS
- 21. Exhibit 21. Distribution of 10-Year Impact on Spending from All-Payer Provider Payment Methods and Rates -$122.4 $0.0 $0.0 -$17.7 -$104.7 -$140 -$120 -$100 -$80 -$60 -$40 -$20 $0 $20 $40 $60 Systemwide Federal Gov't State and Local Gov't Private Payer Households Source: Based on estimates by The Lewin Group for The Commonwealth Fund, 2007. Dollars in billions SAVINGSCOSTS
- 22. Exhibit 22. Distribution of 10-Year Impact on Spending from Limit on Payment Updates in High-Cost Areas -$157.8 -$259.7 $62.1 $27.3$12.6 -$300 -$250 -$200 -$150 -$100 -$50 $0 $50 $100 $150 Systemwide Federal Gov't State and Local Gov't Private Payer Households Source: Based on estimates by The Lewin Group for The Commonwealth Fund, 2007. Dollars in billions SAVINGSCOSTS
- 23. Exhibit 23. Cumulative Changes in Annual National Health Expenditures, 2000–2007 0 25 50 75 100 125 2000 2001 2002 2003 2004 2005 2006* 2007* Net cost of private health insurance administration Family private health insurance premiums Personal health care Workers earnings Notes: Data on premium increases reflect the cost of health insurance premiums for a family of four/the average premium increase is weighted by covered workers. * 2006 and 2007 private insurance administration and personal health care spending growth rates are projections. Sources: A. Catlin, C. Cowan, S. Heffler et al., “National Health Spending in 2005: The Slowdown Continues,” Health Affairs, Jan./Feb. 2007 26(1):143–53; J. A. Poisal, C. Truffer, S. Smith et al., “Health Spending Projections Through 2016: Modest Changes Obscure Part D’s Impact,” Health Affairs Web Exclusive (Feb. 21, 2007):w242–w253; Henry J. Kaiser Family Foundation/Health Research and Educational Trust, Employer Health Benefits Annual Surveys, 2000–2007 (Washington, D.C.: KFF/HRET). 109% 65% 91% 24% Percent change
- 24. Exhibit 24. Cumulative Impact on National Health Expenditures (NHE) of Insurance Connector Approach Plus Selected Individual Options $31 $1,554 $1,258 $997 $770 $573 $407 $84 $163 $272 $0 $400 $800 $1,200 $1,600 $2,000 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 Cumulative impact Annual net impact Dollars in billions Note: Selected individual options include improved information, payment reform, and public health. Source: Based on projected expenditures absent policy change and Lewin estimates. SavingstoNHE
- 25. Exhibit 25. Net Federal Spending with Insurance Connector Alone Compared with Net Federal with Insurance Plus Savings Options $50 $109 $195 $10$13 $31 $0 $50 $100 $150 $200 $250 2008 2012 2017 Federal spending offset Net federal with insurance plus savings options*Dollars in billions * Selected options include improved information, payment reform, and public health. Source: Lewin Group modeling estimates of insurance option alone or insurance in combination with savings options compared with projected federal spending under current policies. $82 Insurance Alone $122 Insurance Alone $205 Insurance Alone
- 26. Exhibit 26. Total National Health Expenditures, 2008–2017 Projected and Various Scenarios 3.0 3.2 3.4 3.6 3.9 4.1 4.4 2.3 2.8 2.6 2.4 2.9 3.0 3.2 3.4 3.7 3.9 4.1 2.7 3.6 3.4 3.3 3.1 3.0 2.8 2.6 2.5 2.4 2.9 $2.0 $2.5 $3.0 $3.5 $4.0 $4.5 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 Projected under current system Insurance Connector plus selected individual options* Spending at current proportion (16.2%) of GDP * Selected individual options include improved information, payment reform, and public health. Source: Based on projected expenditures absent policy change and Lewin estimates. Dollars in trillions