Download to read offline












































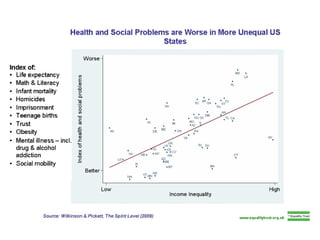



The document criticizes the U.S. medical system as being the most ineffective, unjust, inequitable and unethical among wealthy nations. It argues that the 2009 health reforms made the system worse. It provides examples showing racial and socioeconomic disparities in access to healthcare and health outcomes. It also discusses issues like the high costs of the system, medical bankruptcy, and how viewing patients as consumers is problematic.



































































