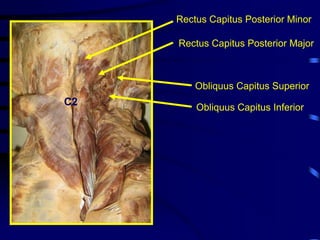
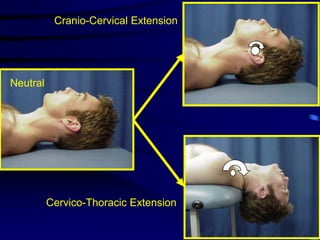
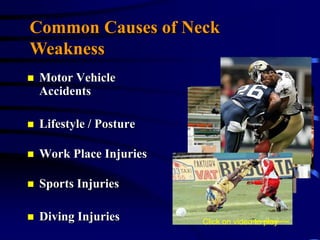
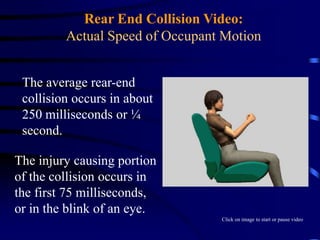
This document summarizes a presentation given by Marc Weinberg, D.C. on cervical spine muscular weakness. It discusses the anatomy of cervical flexors and extensors, common causes of neck weakness like motor vehicle accidents, and research showing neck pain is related to muscular weakness. The research presented indicates patients with neck pain have significantly weaker neck muscles than healthy subjects, and strengthening exercises are an important part of neck rehabilitation.

![ResearchQuantitative cervical flexor strength in healthy subjects and in subjects with mechanical neck pain ARCH PHYS MED REHABIL 1991AUG; 72(9) pp. 679 - 81 Silverman J, Rodriquez A, Agre J, Alta Bates-Herrick Hospital, Berkeley, CA [Anterior cervical muscle] weakness and its role in persistent neck pain should be recognized. The efficiency and effect of cervical muscle strengthening in treatment of chronic neck pain should be further defined.](https://image.slidesharecdn.com/sccapresentation-110719142530-phpapp02/85/SCCA-Presentation-46-320.jpg)