
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Dermatomyositis
Similar to Dermatomyositis (20)
More from Harsh shaH
More from Harsh shaH (20)
Recently uploaded
Recently uploaded (20)
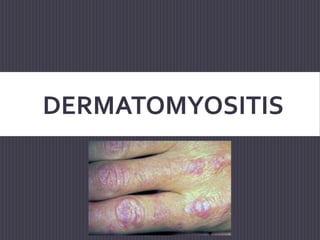
Dermatomyositis
- 2. DERMATOMYOSITIS Dermatomyositis (DM) is a chronic inflammatory disorder of the skin and muscles. An autoimmune disease Skin involvement in DM usually manifests with characteristic papules over digits, erythema over the elbows and knees, a heliotrope rash around the eyes, periungual telangiectasias, and dystrophic cuticles. Muscle involvement usually manifests as proximal muscle weakness initially, with or without myalgias or tenderness.
- 3. AMYOPATHIC DERMATOMYOSITIS Amyopathic dermatomyositis can be a challenging diagnosis because patients lack traditional muscle findings. "Clinically amyopathic" dermatomyositis (CADM) accounts for the presence of subclinical muscle disease in some of these patients. These patients represent a substantial minority of dermatomyositis cases and have similar co-morbidities to "classic" dermatomyositis patients, including interstitial lung disease and malignancy. Clinically amyopathic dermatomyositis patients should not be considered as a distinct clinical entity from "classic" dermatomyositis, as they share antibody sub-types and associated co-morbidities, likely representing clinical spectrum of a common disease.
- 4. DESCRIPTION Dermatomyositis occurs more commonly in female patients. There are 2 types of DM: adult onset type & juvenile type. It presents as a proximal symmetrical muscle weakness with vasculitis affecting the skin, muscles and internal organs. Patients find it hard to raise their arms to comb their hair or walk up the stairs due to the proximal muscle weakness. It can be severe enough to affect the muscles needed for speech and swallowing and is also known to cause respiratory compromise.
- 5. EPIDEMIOLOGY The estimated incidence of dermatomyositis is 9.63 cases per million population. The estimated incidence of AMD is 2.08 cases per million. Dermatomyositis can occur in people of any age. Two peak ages of onset exist: in adults, the peak age of onset is approximately 50 years, whereas in children, the peak age is approximately 5-10 years. Dermatomyositis and polymyositis are twice as common in women as in men. Neither condition shows any racial predilection
- 6. CAUSE The cause of dermatomyositis is unknown. However, genetic, immunologic, infectious, and environmental factors have been implicated. Infectious agents have been suggested as possible triggers of dermatomyositis. These include the following: 1. Viruses (eg, coxsackievirus, parvovirus, echovirus, human T-cell lymphotropic virus type 1 [HTLV-1], HIV) 2. Toxoplasma species 3. Borrelia species
- 7. CAUSE Cases of drug-induced dermatomyositis have been reported. Dermatomyositis-like skin changes have been reported with hydroxyurea in patients with chronic myelogenous leukemia or essential thrombocytosis.
- 8. AGENTSTHAT MAYTRIGGERTHE DISEASE Statins Penicillamine Anti–tumor necrosis factor drugs Anti–programmed cell death drugs [28] Interferon Cyclophosphamide Bacillus Calmette-Guérin (BCG) vaccine Quinidine
- 9. IMMUNOPATHOGENESIS DM is an immune-mediated disorder, with proven immunohistopathology and response to immunosuppression. The typical histopathologic findings of DM in muscle include perifascicular atrophy, endothelial cell swelling, vessel wall membrane attack complex (MAC) deposition, capillary necrosis, infarcts, major histocompatibility complex (MHC) I upregulation, and the presence of an inflammatory infiltrate consisting of T and B lymphocytes, macrophages, and plasma cells.
- 10. IMMUNOPATHOGENESIS There are findings of predominant perimysial and perivascular B/CD4+ T cell infiltrate and intravascular MAC deposition. Recent studies have provided evidence that 30–90% of the CD4+ cells found in DM muscle are actually plasma cytoid dendritic cells. The typical histopathologic findings in DM skin include epidermal basal cell vacuolar degeneration, apoptosis of epidermal basal and suprabasal cells often with epidermal atrophy, and increased dermal mucin deposition. Features that are more specific to DM over cutaneous lupus include C5b-deposition in both dermal vasculature and the dermal-epidermal junction and a perivascular lymphocytic infiltrate.
- 11. IMMUNOPATHOGENESIS DM has traditionally been viewed as a humorally mediated vasculopathic disease given the findings of autoantibodies and complement deposition in vessels. The proposed mechanism has been that binding of antibodies targeting the endothelium of the endomysial capillaries leads to activation of the complement system with subsequent MAC deposition. This in turn may lead to endothelial swelling, capillary necrosis, perivascular inflammation, and muscle ischemia. Relative hypoperfusion of the perifascicular regions is thought to explain the findings of atrophy in this region on muscle biopsy.
- 12. CLINICAL MANIFESTATIONS Muscle disease Skin disease Lung disease
- 13. MUSCLE DISEASE DM presents with a varying degree of muscle weakness that is insidious in onset and gradually worsens over weeks to months, but a more fulminant progression can occur. The initial presentation of muscle involvement is typically symmetric and proximal, with distal muscle weakness occurring late in the course of the disease. Patients often have difficulty with activities such as rising from a chair, climbing stairs, lifting objects, or washing their hair.
- 14. MUSCLE DISEASE Difficulty holding and manipulating objects can occur with distal muscle involvement. When the neck extensor muscles are involved, patients can present with head drop. With more severe disease, patients can develop dysphagia, dysphonia, and weakness in the muscles of respiration. Myalgias and muscle tenderness are less common but can occur in up to 30% of patients.
- 15. SKIN DISEASE The characteristic rash of DM can occur before, shortly after, or at the same time as muscle weakness. A hallmark sign of DM are Gottron's papules
- 16. GOTTRON’S PAPULES These lesions primarily consist of erythematous to violaceous papules and plaques over the extensor surfaces of the metacarpophalangeal and interphalangeal joints. These lesions may have accompanying scale, and can sometimes develop ulcerations; active lesions tend to resolve with dyspigmentation, atrophy, and scarring. • Gottron's sign refers to erythematous macules and patches overlying the elbows and/or knees, and are less specific findings for DM
- 17. SKIN DISEASE Another hallmark sign of DM is the heliotrope rash which consists of violaceous erythema of the upper eyelids often with associated edema and telangiectasia. It should be noted that in darker skin types, this erythema may be subtle and overlooked. Erythematous patches and/or plaques in other characteristic sun-exposed or nonsun-exposed areas may also be seen in DM.
- 18. HELIOTROPE RASH A confluent erythema in the malar distribution involving the cheeks and extending over the nasal bridge may be seen, and can often involve the nasolabial folds. More extensive involvement can be seen in other areas including the forehead, lateral face, and ears. Confluent macular erythema over the lower anterior neck and upper anterior chest can also be seen (the so-called “V” sign)
- 19. SKIN DISEASE A shawl sign refers to erythema over the upper back, posterior neck, and shoulders, sometimes with extension to the lateral arms (figure d) Nonsun-exposed areas can also be involved, especially the sclap, lower back, and lateral thighs (Holster sign). (figure e)
- 20. VASCULOPATHIC LESIONS Vasculopathic lesions of DM include livedo reticularis, ulceration, and telangiectasia (including gingival and periungual). On nailfold capillary examination, DM patients can have prominent dilated and tortuous blood vessels accompanied by avascular areas. The degree of telangiectasias and vessel drop-out reflects ongoing disease activity, particularly in the skin.
- 21. VASCULOPATHIC LESIONS (a) Shallow, crusted erosions arising in an area of intense inflammation. (b) Telangiectatic macules and papules on the breast in a patient with longstanding disease
- 22. HAND LESIONS Rough and cracked, hyperkeratotic, “dirty” horizontal lines on the lateral and palmer areas of the fingers, resembling “mechanics” hands. Cuticular overgrowth and irregularity on the nail plate. Palmar and plantar erythema occasionally associated with a mottled appearance may be indicative of vascular instability in DM patients. In addition, raised, often tender papules or plaques can be present overlying joint creases of the palmar hands. On biopsy, these lesions demonstrate mucin deposition in the dermis.
- 23. HAND LESIONS (a) Mechanic hands: Erythematous, scaling papules located on the lateral aspect of the second and third digits. (b) Overgrown cuticles are seen containing multiple hemorrhages.
- 24. OTHER CUTANEOUS FEATURES Other potentially significant cutaneous features of DM include panniculitis, alopecia (focal, due to areas of inflammation on the scalp, or diffuse), and flagellate erythema (linear streaks in the upper back occurring in association with excoriations from pruritus). Poikiloderma is a manifestation of disease chronicity with a mottled pattern of hyperpigmented and hypopigmented macules interspersed with telangiectasias. Lastly, calcinosis involving the skin, subcutaneous tissue, fascia, or muscle seen in areas of potential trauma or inflammation is often a late complication, seen more often in juvenile than in adult cases.
- 25. LUNG DISEASE ILD is a significant source of morbidity and mortality in patients with inflammatory myositis. It has been estimated that about 35–40% of patients with either polymyositis or dermatomyositis will suffer from ILD during the course of their illness. Large case series have suggested that over 75% of patients who have an anti- synthetase antibody will develop ILD, however, a small prospective longitudinal study suggested that anti-Jo antibody positivity may portend a better ILD prognosis.
- 26. INERSTITIAL LUNG DISEASE(ILD) Pulmonary function testing typically reveals a restrictive disease pattern (forced vital capacity [FVC] or total lung capacity [TLC] <80% predicted for age) or a decrease in diffusing capacity of carbon monoxide (DLCO). High-resolution CT (HRCT) scanning is very sensitive for the detection of ILD and can be helpful to follow disease progression. Characteristic features on HRCT include nodules, linear opacities, fibrosis with or without honeycombing, consolidation, traction bronchiectasis, and bronchiolectasis Bronchoscopy with bronchoalveolar lavage is helpful to rule out occult infections in patients who are chronically immunosuppressed.
- 27. OESOPHAGEAL INVOLVEMENT Esophageal disease in DM patients most commonly presents with dysphagia to solids and liquids due to loss of pharyngo–esophageal muscle tone. Other signs of pharyngo–esophageal involvement include nasal speech, hoarseness, nasal regurgitation, and aspiration pneumonia. A diagnosis can be confirmed by manometry with low amplitude/absent pharyngeal contractions and decreased upper esophageal sphincter pressures
- 28. SYSTEMIC MANIFESTATIONS General systemic disturbances, fever, arthralgia, malaise, weight loss, Raynaud phenomenon Dysphagia due to esophageal skeletal muscle involvement Gastroesophageal reflux due to esophageal smooth muscle involvement Dysphonia Atrioventricular defects, tachyarrhythmias, dilated cardiomyopathies Gastrointestinal ulcers and infections, more common in children Pulmonary involvement due to weakness of thoracic muscles, interstitial lung disease Subcutaneous calcification, which may result in contracture of joints; more common in children Children may also develop a tiptoe gait secondary to flexion contracture of the ankles in early childhood Malignancy in adult patients
- 29. LABORATORYTESTING Muscle enzyme levels Myositis-specific antibodies, Antinuclear antibody levels Pulmonary function studies with diffusion capacity Electrocardiography, Esophageal manometry Colonoscopy to screen for underlying malignancy Papanicolaou smear in women for malignancy screening CA-125 and CA-19-9 for malignancy screening
- 30. DIAGNOSIS In classic DM, in addition to cutaneous manifestations and proximal muscle weakness, patients have abnormal muscle enzymes (creatine kinase [CK], aldolase, aspartate aminotransferase [AST], alanine aminotransferase [ALT], and/or lactate dehydrogenase [LDH]). Electromyogram (EMG) studies are useful early in disease and show abnormal findings in 70–90% of cases but are nonspecific and can be seen in other muscle diseases.
- 31. DIAGNOSIS Typical EMG findings include increased spontaneous and insertional activity with fibrillation potentials, positive sharp waves, complex repetitive discharges, early recruitment, and small polyphasic motor until potentials. Imaging with magnetic resonance imaging (MRI) is a sensitive technique for evaluation of myositis with the presence of muscle edema. Areas of inflammation are hyperintense on T2-weighted images with clearer images seen with fat suppression or short tau inversion recovery sequences
- 32. DIAGNOSIS Muscle and/or skin biopsies are required to make a definite diagnosis and to rule out other disease mimickers. The muscle biopsy should be obtained from moderately weak muscle areas as assessed by physical exam, areas of inflammation located by MRI, or muscles contralateral to those identified as abnormal on EMG.
- 33. BOHAN AND PETER’S CRITERIA
- 36. BIOMARKERS Targets, prevalence, and clinical association of myositis-specific antibodies. ILD: interstitial lung disease;TIF: transcription intermediary factor; RNA: ribonucleic acid; MDA: melanoma differentiation-associated gene; CADM: clinical amyopathic dermatomyositis; NXP: nuclear matrix protein; SAE: small ubiquitin-like modifier-activating enzyme;ARS: aminoacyl tRNA synthetase.
- 37. DIFFERENTIAL DIAGNOSIS Discoid Lupus Erythematosus GraftVersus Host Disease Lichen Myxedematosus Lichen Planus Multicentric Reticulohistiocytosis Parapsoriasis Pityriasis Rubra Pilaris Polymorphous Light Eruption Psoriasis Rosacea Sarcoidosis Subacute Cutaneous Lupus Erythematosus (SCLE) Systemic Lupus Erythematosus (SLE) Tinea Corporis
- 38. PROGNOSIS Dermatomyositis may spontaneously remit in as many as 20% of affected patients. About 5% of patients have a fulminant progressive course with eventual death. However, patients who survive the disease may experience residual weakness and disability. Children with severe dermatomyositis may develop contractures. Therefore, many patients require long-term therapy.
- 39. PROGNOSIS Risk factors for a poorer prognosis in patients with dermatomyositis include the following: An associated malignancy Cardiac, pulmonary, or esophageal involvement Older age (ie, >60 years) Dermatomyositis may cause death because of muscle weakness or cardiopulmonary involvement. Patients with an associated cancer may die of the malignancy.
- 40. PROGNOSIS The association between malignancy and dermatomyositis has long been recognized. An estimated 25% of patients with dermatomyositis have or will develop an associated malignancy, and the risk appears to remain elevated for 3- 5 years.
- 41. TREATMENT Therapy for the muscle component of dermatomyositis involves the use of corticosteroids, typically with an immunosuppressive agent. Therapy for the skin disease includes the following, among other options: Sun avoidance, Sunscreens and photoprotective clothing Topical corticosteroids Antimalarial agents Methotrexate Mycophenolate mofetil Immune globulins
- 42. TREATMENT OF MUSCLE DISEASE The mainstay of therapy for the muscle disease is systemically administered corticosteroids. Traditionally, prednisone (0.5-2 mg/kg/d) up to a dose of 60 mg/d is given as initial therapy. The drug should be slowly tapered to avoid relapse of the disease. Because most patients develop steroid-related toxic effects, most authorities administer a steroid-sparing immunosuppressive or cytotoxic agent early in the course
- 43. TREATMENT OF MUSCLE DISEASE Drugs reported to be steroid-sparing in some patients or in small open-label studies have included the following Methotrexate Azathioprine Cyclophosphamide Cyclosporine Mycophenolate mofetil Leflunomide Chlorambucil Tacrolimus
- 44. TREATMENT OF MUSCLE DISEASE Generally, methotrexate, mycophenolate mofetil, or azathioprine are used first line as glucocorticoid-sparing agents for muscle involvement. Response rates to methotrexate have been reported to be approximately 70-80%. In addition, one small, randomized trial supported the long-term benefits of azathioprine as compared with prednisone monotherapy. Results with cyclophosphamide in severe cases have been disappointing.
- 45. TREATMENT OF MUSCLE DISEASE For refractory cases, the use of monthly high-dose intravenous immune globulin (IVIG) for 6 months has proved beneficial in the short term. In addition to its positive effects on refractory muscle and skin disease, IVIG has been reported to be beneficial for other systemic manifestations, including severe esophageal dysfunction.
- 46. TREATMENT OF MUSCLE DISEASE The calcineurin inhibitor tacrolimus appears to be effective, safe, and well tolerated in patients with dermatomyositis that is refractory to other treatments. In addition to improvement in muscle strength and physical function, amelioration of skin lesions and interstitial lung disease have been reported. However, randomized, controlled trials have yet to be conducted
- 47. TREATMENT OF SKIN DISEASE Therapy of cutaneous disease of dermatomyositis is often difficult First-line therapy is to recognize that the patient is photosensitive and to prescribe sun avoidance and sun protection measures, including broad- spectrum sunscreens and photoprotective clothing. The cutaneous component of dermatomyositis is exacerbated by sunlight and other sources of ultraviolet light; in addition, the muscle component may be exacerbated.
- 48. TREATMENT OF SKIN DISEASE Hydroxychloroquine and chloroquine have been beneficial in small, open- label case studies; however, roughly 25-30% of patients with dermatomyositis who are treated with hydroxychloroquine develop a drug eruption, and patients should be counseled regarding this potential side effect. Some patients who develop a drug eruption to hydroxychoroquine may go on to tolerate chloroquine
- 49. TREATMENT OF SKIN DISEASE Methotrexate is often considered first-line systemic therapy if antimalarials fail or are contraindicated. Mycophenolate mofetil has been reported to be useful as well. Azathioprine has been reported to be effective for muscle involvement, but Azathioprine appears to be less effective for cutaneous disease. Sirolimus, tactrolimus, and dapsone inhibitors are among other immunomodulatory medications that may be of value in some patients.
- 50. TREATMENT OF SKIN DISEASE Intravenous immune globulin (IVIG) has benefited muscle involvement and cleared the skin lesions in the patients in whom it was used. A study found that muscular and cutaneous involvement were significantly improved at 6 months in the IVIG-treated group, and modified Cutaneous Dermatomyositis Area and Severity Index (CDASI) scores were significantly improved over pretreatment scores during 4 years of follow-up Subcutaneous IgG has also been effective in dermatomyositis. Rituximab has been used for skin disease, but the results are mixed.
- 53. REFERENCES 1. Indian J Dermatol. 2012 Sep-Oct; 57(5): 375–381 2. Hindawi Journal of Immunology Research Volume 2019, Article ID 9141420, 15 pages https://doi.org/10.1155/2019/9141420 3. Dalakas MC and Hohlfeld R, Lancet 362:971-82, 2003 4. Bohan A and Peter JB, N Engl J Med. 292:344-7, 1975; Bohan A and Peter JB, N Engl J Med. 292:403-7, 1975 5. Hautarzt. 2015 Aug;66(8):604-10. 6. Current Rheumatology Reports (2019) 21:53 https://doi.org/10.1007/s11926-019-0850-9 7. Medscape dermatomyositis