![Introduction:
• The term ‘small round-cell tumour’ (SRCT) traditionally describes a group of
undifferentiated paediatric tumours that can present diagnostic difficulty because they may
be indistinguishable using light microscopy. [Aidan P. Mcmanus, Barry A. Gusterson. The Molecular Pathology Of
Small Round-cell Tumours-relevance To Diagnosis, Prognosis, And Classification. Journal Of Pathology, Vol. 178: 116--121 (1996)])
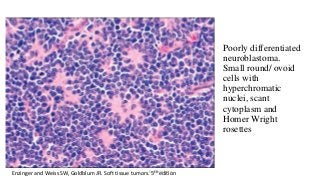
• Small round cell Tumors are a group of cytomorphologically similar neoplasm with
varied orgin. The neoplastic elements include undifferentiated , uniform, small round
to oval closely packed cells with a solitary hyperchromatic nucleus and a high nuclear
cytoplasmic ratio. The nucleoli may or may not be prominent. (Reshma Et al. Small round cell
tumor of head and neck region.International journal of oral and maxillofacial pathology.2014)
• Heterogeneous group of neoplasms featuring primitive, undifferentiated round-cell
morphology
• Therefore often lacking any particular morphological features that would allow precise
identification.
Dr.Aldrin Jerry](https://image.slidesharecdn.com/roundcelltumors-170909125355/85/Round-cell-tumors-3-320.jpg?cb=1718505216)
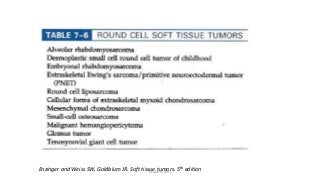



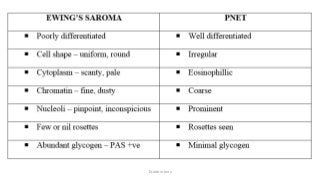

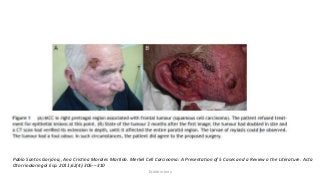




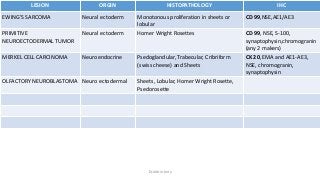

The document discusses various types of small round cell tumors (SRCTs) primarily found in children, including their classification, characteristics, and clinical features. It details individual tumors such as Ewing's sarcoma, rhabdomyosarcoma, and Merkel cell carcinoma, along with their ages, histopathological features, and treatment options. The document emphasizes the diagnostic challenges posed by these tumors due to their cytomorphological similarities and varying origins.









































































