ROLE OF HCG IN DEFINITIVE DIAGNOSIS-A CASE STUDY, ACBICON 2008
•
1 like•395 views

This case study presents the diagnostic challenges of a 24-year old woman who presented with fever and abnormal bleeding at 8 weeks of pregnancy. Beta human chorionic gonadotropin (β hCG) levels, ultrasound findings, and histology were inconclusive between diagnoses of hydropic abortion versus partial molar pregnancy. The patient underwent dilation and evacuation followed by normalization of β hCG levels over weeks, confirming a diagnosis of hydropic abortion. The case highlights how β hCG levels can aid in differentiating conditions when imaging and histology are non-diagnostic.
Recommended

Recommended
More Related Content
Viewers also liked
Viewers also liked (16)
Similar to ROLE OF HCG IN DEFINITIVE DIAGNOSIS-A CASE STUDY, ACBICON 2008
Similar to ROLE OF HCG IN DEFINITIVE DIAGNOSIS-A CASE STUDY, ACBICON 2008 (20)
More from Moushumi Lodh, MD
More from Moushumi Lodh, MD (9)
Recently uploaded
Recently uploaded (20)
ROLE OF HCG IN DEFINITIVE DIAGNOSIS-A CASE STUDY, ACBICON 2008
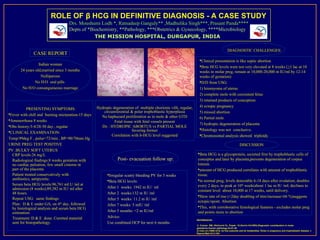
- 1. ROLE OF β HCG IN DEFINITIVE DIAGNOSIS - A CASE STUDY Drs. Moushumi Lodh *, Ratnadeep Ganguly** ,Madhulika Singh***, Prasant Panda**** Depts of *Biochemistry, **Pathology, ***Obstetrics & Gynecology, ****Microbiology THE MISSION HOSPITAL, DURGAPUR, INDIA 1 2 1 2 DIAGNOSTIC CHALLENGES: CASE REPORT 1 2 1 2 Clinical presentation is like septic abortion Indian woman Beta HCG levels were not very elevated at 8 weeks (>1 lac at 10 24 years old,married since 3 months weeks in molar preg, remain at 10,000-20,000 m IU/ml by 12-14 Nulliparous weeks of gestation) No H/O oral pills D/D from USG: No H/O consanguineous marriage 1) leiomyoma of uterus 2) complete mole with coexistent fetus 3) retained products of conception Hydropic degeneration of multiple chorionic villi, regular, 4) ectopic pregnancy PRESENTING SYMPTOMS: circumferential & polar trophoblastic hyperplasia 5) missed abortion Fever with chill and burning micturation-15 days No haphazard proliferation as in mole & other GTD 6) Partial mole Amenorrhoea 8 weeks Fetal tissue with fetal vessels present 7) hydropic degeneration of placenta Obs history:3-4/28-30 day , regular Dx : HYDROPIC ABORTUS vs PARTIAL MOLE favoring former Histology was not conclusive. CLINICAL EXAMINATION: a Correlation with b-HCG level suggested Chromosomal analysis showed triploidy Temp:99deg F , pulse=72/min , BP=90/70mm Hg URINE PREG TEST POSITIVE DISCUSSION PV :BULKY SOFT UTERUS CRP levels:26 mg/L Beta HCG is a glycoprotein, secreted first by trophoblastic cells of Radiological findings:8 weeks gestation with Post- evacuation follow up: conceptus and later by placenta,prevents degeneration of corpus no cardiac pulsation, few small cisterns in luteum. part of the placenta amount of HCG produced correlates with amount of trophoblastic Patient treated conservatively with Irregular scanty bleeding PV for 3 weeks tissue. antibiotics, antipyretic. Beta HCG levels: in normal preg, levels detectable 6-18 days after ovulation; doubles Serum beta HCG levels:96,761 mI U /ml at every 2 days, to peak at 10th week(about 1 lac m IU /ml; declines to admission (8 weeks);89,382 m IU/ ml after After 1 weeks: 1942 m IU/ ml constant level about 10,000 at 17 weeks, until delivery. 48 hours. After 2 weeks:132 m IU /ml Slow rate of rise (<2day doubling of titre/increase<66 %)suggests 1 2 Repeat USG: same findings After 5 weeks: 11.2 m IU /ml ectopic/spont. Abortion Plan: D & E under GA, on 4 day, followed th After 7 weeks: 5 mIU /ml by histological analysis and serum beta HCG This, with corroborative histological features - excludes molar preg 1 2 34 5 6 estimation. After 5 months: <2 m IU/ml and points more to abortion Treatment: D & E done. Curetted material Advice: REFERENCES: sent for histopathology. Use combined OCP for next 6 months 1) Conran RM, Hitchcock CL, Popek EJ,Norris HJ(1993).Diagnostic consideration in molar gestations.Human pathology,24;41-48 2) Cole LA (1998) hCG, its free subunits and its metabolites. Roles in pregnancy and trophoblastic disease. J Reprod Med 43:3-10H