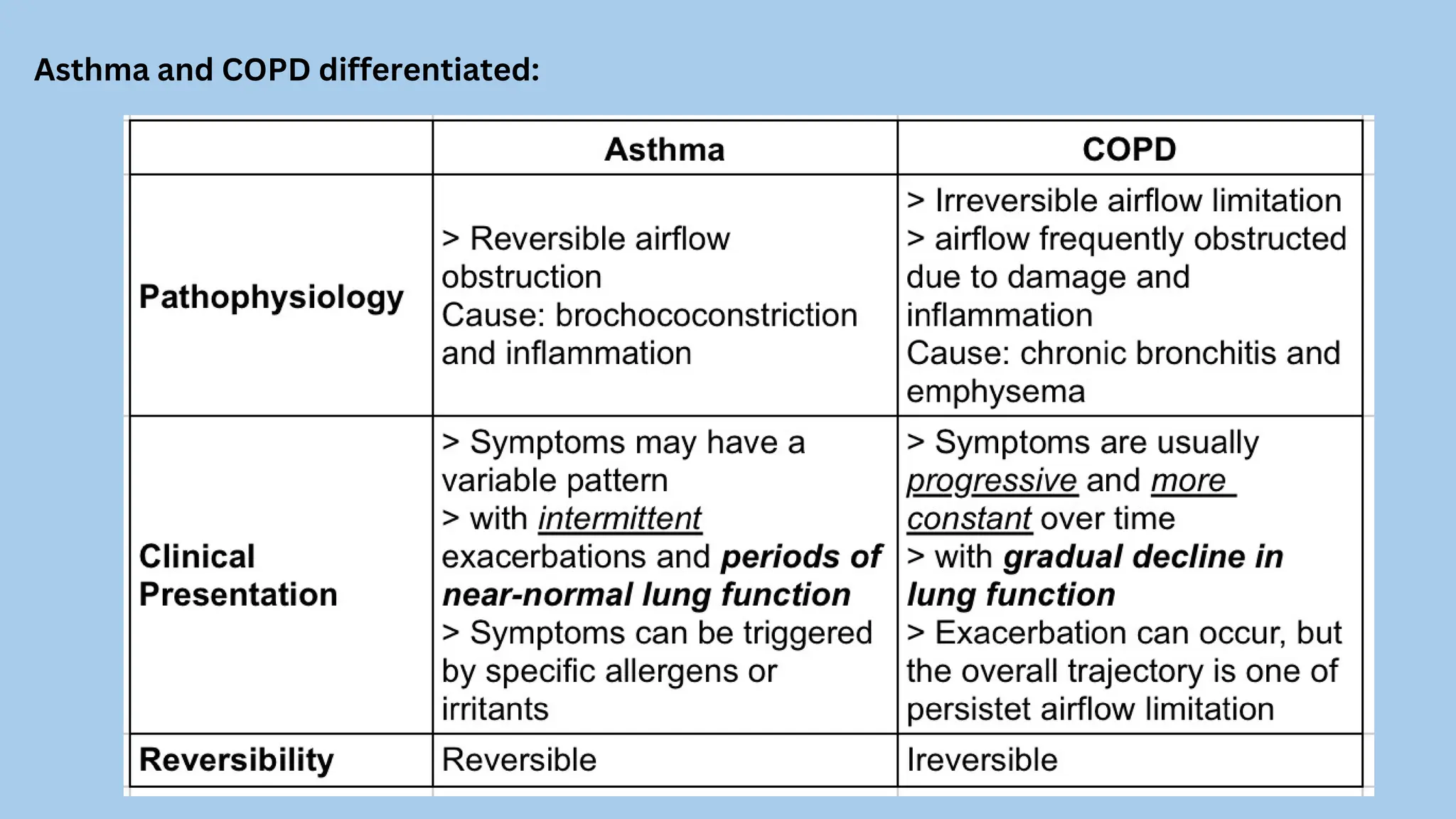
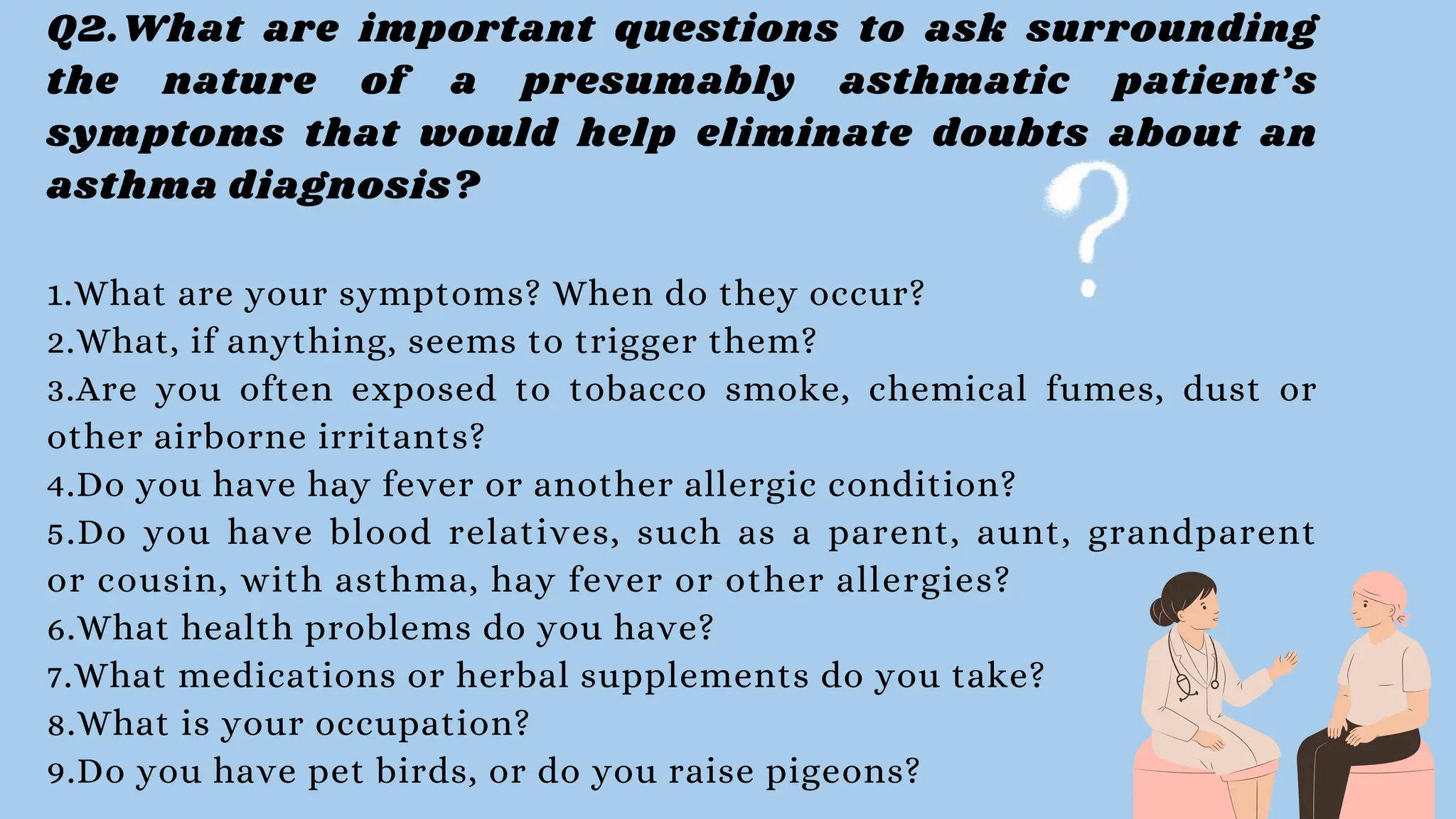
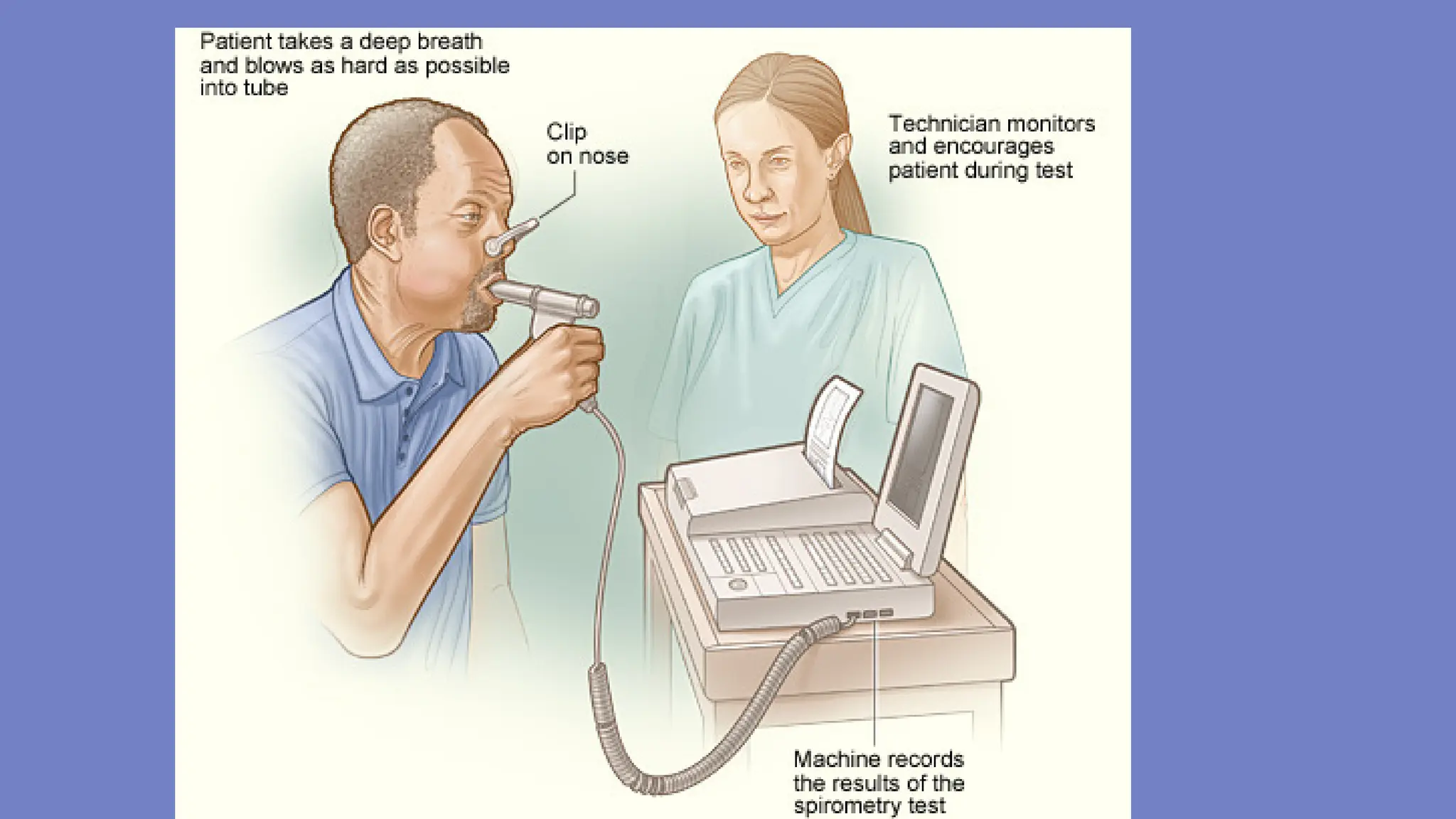
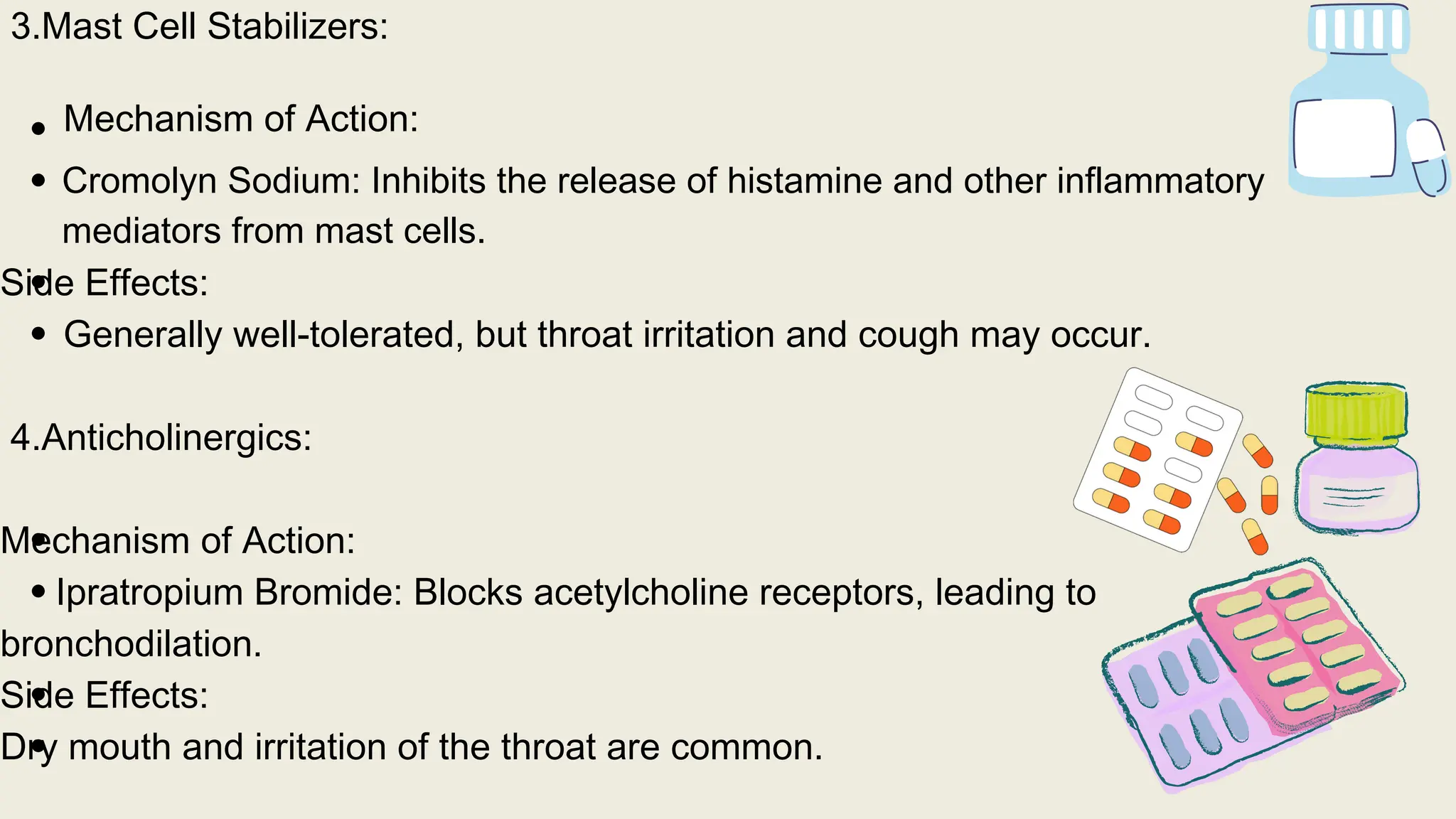
The document discusses a case of a 23-year-old female presenting with shortness of breath and cough after exposure to a cat, detailing her medical history and vital signs. It explains asthma's pathophysiology, diagnosis, and differentiation from COPD, emphasizing the importance of spirometry for diagnosis and inhaled corticosteroids as first-line treatment. The therapeutic plan includes trigger avoidance, asthma education, and regular follow-ups to enhance asthma management and reduce exacerbations.







































![Microsoft PowerPoint - Asthma 4th year Lecture (1) [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/microsoftpowerpoint-asthma4thyearlecture1compatibilitymode-220716165932-01cf3f8c-thumbnail.jpg?width=640&height=640&fit=bounds)
![Microsoft+PowerPoint+-+Asthma+4th+year+Lecture+(1)+[Compatibility+Mode].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/microsoftpowerpoint-asthma4thyearlecture1compatibilitymode-230704125445-487a63ed-thumbnail.jpg?width=640&height=640&fit=bounds)






















