DEFINITION
• Regional anaesthesiainvolves blocking sensation to a
specific region of the body.
• Spinal anaesthesia is a type of regional anaesthesia in
which a local anaesthetic agent is injected into the
subarachnoid space (i.e., the cerebrospinal fluid-filled
space between the arachnoid and pia mater) to produce a
temporary, reversible loss of sensation and motor function
in the lower part of the body
• Epidural anaesthesia is a form of regional anaesthesia in
which a local anaesthetic is injected into the epidural space
(the space outside the dura mater) of the spinal cord,
resulting in segmental loss of sensation and/or motor
function in the body below the level of injection.
4.
Mechanism of Action
•- Both techniques block transmission of nerve
impulses by inhibiting sodium channels.
• - Spinal: Directly into CSF in subarachnoid
space.
• - Epidural: Injected into epidural space
surrounding dura mater.
• - Result: Sensory, motor, and sympathetic
block.
5.
Pathophysiology of RegionalAnaesthesia
• - Spinal: Rapid onset due to direct CSF contact.
• - Epidural: Slower onset; diffusion across dura
to reach spinal nerves.
• - Sympathetic blockade: Causes vasodilation,
hypotension, and bradycardia.
6.
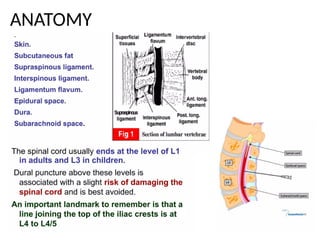
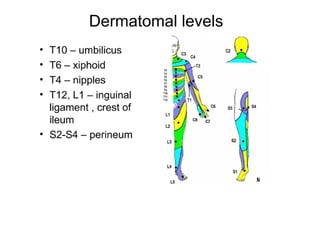
Relevant Anatomy
• -Spinal cord ends at L1-L2 in adults.
• - Epidural space: Between ligamentum flavum
and dura mater.
• - Layers: Skin → Subcutaneous tissue →
Ligaments → Epidural space → Dura →
Subarachnoid space.
7.
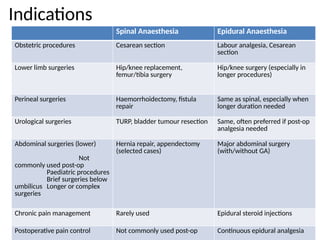
Indications
Spinal Anaesthesia EpiduralAnaesthesia
Obstetric procedures Cesarean section Labour analgesia, Cesarean
section
Lower limb surgeries Hip/knee replacement,
femur/tibia surgery
Hip/knee surgery (especially in
longer procedures)
Perineal surgeries Haemorrhoidectomy, fistula
repair
Same as spinal, especially when
longer duration needed
Urological surgeries TURP, bladder tumour resection Same, often preferred if post-op
analgesia needed
Abdominal surgeries (lower)
Not
commonly used post-op
Paediatric procedures
Brief surgeries below
umbilicus Longer or complex
surgeries
Hernia repair, appendectomy
(selected cases)
Major abdominal surgery
(with/without GA)
Chronic pain management Rarely used Epidural steroid injections
Postoperative pain control Not commonly used post-op Continuous epidural analgesia
• Equipment Checklist
–Sterile spinal tray
– Spinal needle (e.g., 25G Quincke or pencil-point)
– Local anaesthetic (e.g., hyperbaric bupivacaine 0.5%)
– Antiseptic solution (chlorhexidine or povidone-iodine)
– Sterile gloves, drapes, gauze
– Resuscitation equipment and drugs (e.g., ephedrine, atropine)
• Patient Preparation
– Obtain informed consent
– Ensure IV access and preload with fluids (e.g., 500–1000 mL
crystalloids)
– Position patient (sitting or lateral decubitus)
– Monitor: ECG, NIBP, SpO₂
16.
Technique of SpinalAnaesthesiaa
• Positioning Sitting position: patient flexes back (like "mad cat" posture)
• Identification of Insertion Site
– Palpate iliac crests (Tuffier’s line) to identify L3–L4 or L4–L5 interspacec.
• Procedure Steps
– Aseptic technique: clean skin, apply sterile drapes
– Infiltrate skin with local anaesthetic
– Insert spinal needle midline or paramedian
– Advance slowly: feel for "pop" as needle enters dura mater
– Confirm CSF flowInject local anaesthetic slowly (e.g., 2.5–3 mL of 0.5% bupivacaine)
– Withdraw needle and apply dressing
– Position patient according to desired block level.
Post-ProcedureMonitor vitals continuouslyAssess sensory and motor blockWatch for
hypotension, bradycardia, high spinal blockProvide oxygen and vasopressors if needed
17.
A. Patient Evaluation:
•History & Physical Exam: Coagulopathy, infection, spinal deformity, allergies
(especially to local anesthetics), neurologic disease.
• Informed Consent: Explain procedure, risks (e.g. hypotension, post-dural puncture
headache, epidural hematoma), and alternatives.
• Investigations: Check platelet count and coagulation profile if indicated.
B. Equipment Required:
• Sterile gloves, mask, gown, drapes
• Epidural kit:
• Tuohy needle (usually 17–18G)
• Epidural catheter (multi-orifice)
• Loss-of-resistance (LOR) syringe (with saline or air)
• Antiseptic solution (e.g., chlorhexidine)
• Local anesthetic (e.g., lidocaine 2%, bupivacaine 0.25–0.5%)
• Test dose (often lidocaine with epinephrine)
19.
• 2. ProcedureTechnique
• A. Patient Positioning:
• Sitting or lateral decubitus position with maximal lumbar flexion.
• Ensure proper alignment to open the intervertebral spaces.
• B. Identification of Space:
• Typically between L2–L3 or L3–L4 interspaces.
• Use surface landmarks (iliac crests align with L4 vertebral body).
• C. Aseptic Technique:
• Clean skin with antiseptic and drape the area.
• Infiltrate skin and deeper tissues with local anesthetic.
• D. Needle Insertion (Loss-of-Resistance Technique):
• Insert the Tuohy needle in the midline (or paramedian if needed).
• Advance slowly with continuous or intermittent pressure on the LOR syringe.
• Sudden loss of resistance indicates entry into the epidural space.
• E. Catheter Placement:
• Thread the epidural catheter 3–5 cm into the epidural space.
• Remove the Tuohy needle carefully, leaving catheter in place.
• Secure catheter with adhesive dressing.
• F. Test Dose:
• Inject 3 mL of 1.5% lidocaine + epinephrine (1:200,000).
• Look for signs of intrathecal injection (numbness, motor block) or intravascular injection (tachycardia).
• G. Anesthetic Administration:
• Administer the calculated dose of local anesthetic (with or without opioids).
• Titrate dose based on desired level and duration of block.
20.
• 3. Post-ProceduralCare:
• Monitor:
• Blood pressure (risk of hypotension from sympathetic block)
• Heart rate, respiratory status
• Neurologic signs (ensure no motor block if not intended)
• Maintain aseptic technique throughout use.
• Remove catheter if no longer needed or if signs of infection occur.
• Complications (to monitor for):
• Hypotension
• Accidental dural puncture (leading to post-dural puncture headache)
• Epidural hematoma
• Nerve injury
• Catheter misplacement or migration
• Infection (e.g., epidural abscess)
• Would you like a visual diagram or step-by-step illustration of the technique as well?
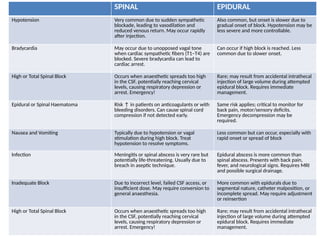
SPINAL EPIDURAL
Hypotension Verycommon due to sudden sympathetic
blockade, leading to vasodilation and
reduced venous return. May occur rapidly
after injection.
Also common, but onset is slower due to
gradual onset of block. Hypotension may be
less severe and more controllable.
Bradycardia May occur due to unopposed vagal tone
when cardiac sympathetic fibers (T1–T4) are
blocked. Severe bradycardia can lead to
cardiac arrest.
Can occur if high block is reached. Less
common due to slower onset.
High or Total Spinal Block Occurs when anaesthetic spreads too high
in the CSF, potentially reaching cervical
levels, causing respiratory depression or
arrest. Emergency!
Rare; may result from accidental intrathecal
injection of large volume during attempted
epidural block. Requires immediate
management.
Epidural or Spinal Haematoma Risk ↑ in patients on anticoagulants or with
bleeding disorders. Can cause spinal cord
compression if not detected early.
Same risk applies; critical to monitor for
back pain, motor/sensory deficits.
Emergency decompression may be
required.
Nausea and Vomiting Typically due to hypotension or vagal
stimulation during high block. Treat
hypotension to resolve symptoms.
Less common but can occur, especially with
rapid onset or spread of block
Infection Meningitis or spinal abscess is very rare but
potentially life-threatening. Usually due to
breach in aseptic technique.
Epidural abscess is more common than
spinal abscess. Presents with back pain,
fever, and neurological signs. Requires MRI
and possible surgical drainage.
Inadequate Block Due to incorrect level, failed CSF access, or
insufficient dose. May require conversion to
general anaesthesia.
More common with epidurals due to
segmental nature, catheter malposition, or
incomplete spread. May require adjustment
or reinsertion
High or Total Spinal Block Occurs when anaesthetic spreads too high
in the CSF, potentially reaching cervical
levels, causing respiratory depression or
arrest. Emergency!
Rare; may result from accidental intrathecal
injection of large volume during attempted
epidural block. Requires immediate
management.
23.
• Definition :
Post-duralpuncture headache (PDPH) is a positional headache that
occurs after a dural puncture, most commonly seen after spinal
anaesthesia or accidental dural puncture during epidural
anaesthesia. It is characterized by a headache that worsens when
sitting or standing and improves when lying flat.2.
• Pathophysiology
Caused by leakage of cerebrospinal fluid (CSF) from the
subarachnoid space through the puncture site in the dura
mater.This loss of CSF volume and pressure leads to:Traction on
pain-sensitive structures in the brain (meninges, cranial
nerves).Cerebral vasodilation due to compensatory mechanisms,
which may also contribute to pain.The larger the dural hole (e.g.,
with larger or cutting needles), the higher the risk.
24.
Signs and Symptoms
•Headache:Positional (worse on standing, better lying
flat)Usually starts 12–72 hours after dural puncture
• Located in frontal, occipital or generalized regions
• Associated symptoms:Neck stiffness, Nausea and
vomiting, disturbances (e.g., diplopia due to cranial
nerve VI palsy in severe cases)
Risk Factors
• Young age (especially females under 40)
• Pregnancy
• Use of large gauge or cutting spinal needles
• Multiple puncture attempts
25.
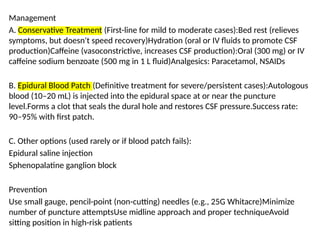
Management
A. Conservative Treatment(First-line for mild to moderate cases):Bed rest (relieves
symptoms, but doesn't speed recovery)Hydration (oral or IV fluids to promote CSF
production)Caffeine (vasoconstrictive, increases CSF production):Oral (300 mg) or IV
caffeine sodium benzoate (500 mg in 1 L fluid)Analgesics: Paracetamol, NSAIDs
B. Epidural Blood Patch (Definitive treatment for severe/persistent cases):Autologous
blood (10–20 mL) is injected into the epidural space at or near the puncture
level.Forms a clot that seals the dural hole and restores CSF pressure.Success rate:
90–95% with first patch.
C. Other options (used rarely or if blood patch fails):
Epidural saline injection
Sphenopalatine ganglion block
Prevention
Use small gauge, pencil-point (non-cutting) needles (e.g., 25G Whitacre)Minimize
number of puncture attemptsUse midline approach and proper techniqueAvoid
sitting position in high-risk patients
26.
Summary
• - Spinaland epidural anaesthesia offer
effective regional blocks.
• - Understanding anatomy and complications
ensures patient safety.
• - PDPH is a common but manageable issue.
• - Pre-assessment and careful technique are
key.













![Central neuraxial block in humans fcps[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/centralneuraxialblockfcps1-250708164057-daf1532a-thumbnail.jpg?width=640&height=640&fit=bounds)
































































