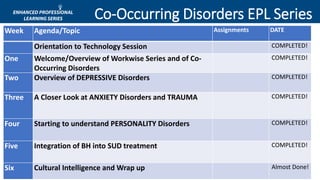
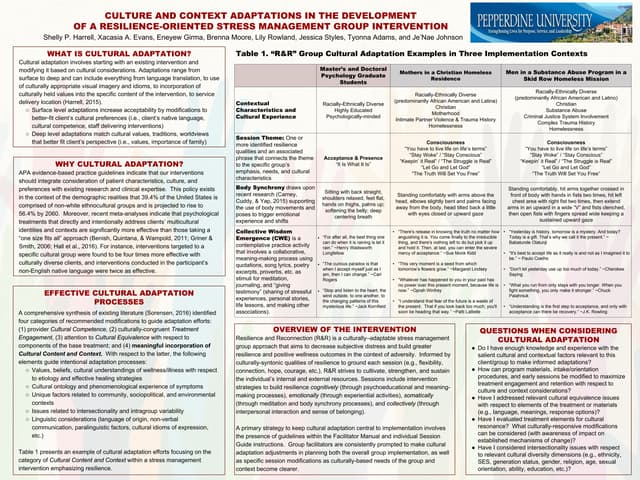
This document provides an agenda and materials for a training session on cultural intelligence and wrapping up a series on co-occurring disorders. The agenda includes reviewing a learning activity on cultural competence, discussing the need for culturally sensitive services, presenting on cultural sensitivity, reviewing and wrapping up the series, and taking final questions. The materials cover topics like cultural competence core elements, reflective practices, engaging diverse clients, contrasting cultural values and behaviors, lessons in cross-cultural dialogue, culturally-informed questions, and treatment implications regarding culture. References include resources on addiction counseling competencies, changing stigma through language, cross-cultural dialogues, and culturally competent treatment.