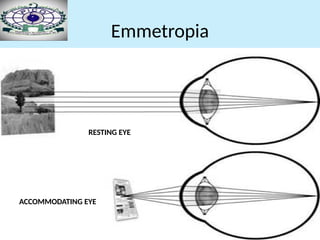
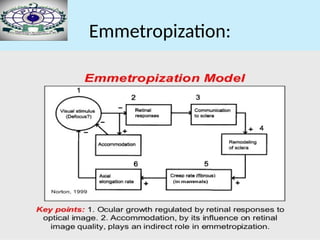
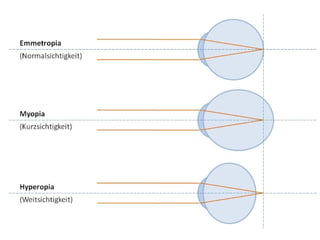
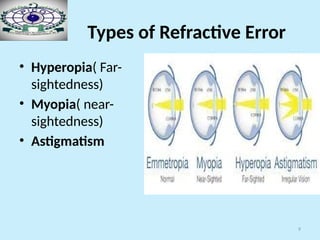
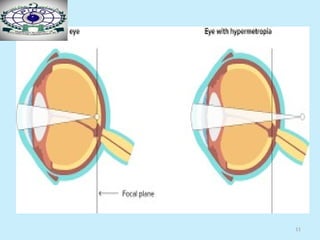
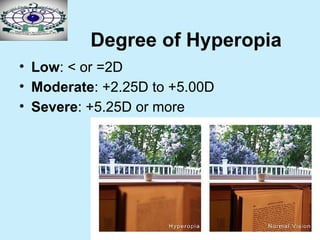
The document discusses the concept of refractive errors, primarily focusing on hyperopia (far-sightedness) and its various types, causes, symptoms, and management strategies. It explains the distinction between emmetropia (normal vision) and ametropia (refractive errors), including classifications of hyperopia based on accommodation and severity. Management recommendations are provided for different age groups, emphasizing optical corrections and therapeutic interventions.