Downloaded 22 times
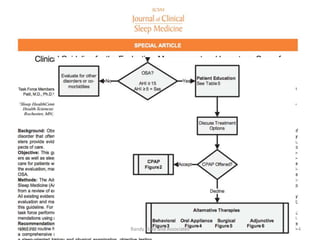
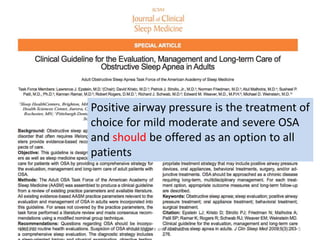
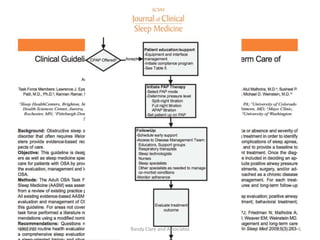
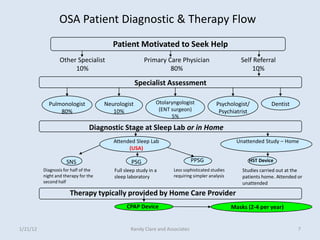


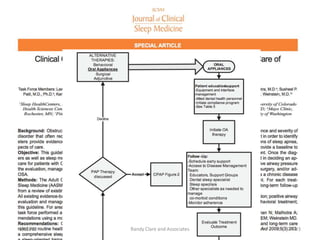
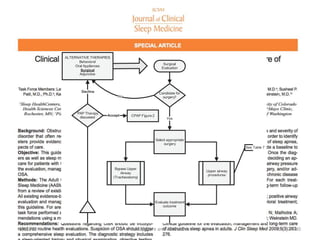

1) The document discusses guidelines for comprehensive sleep therapy, including positive airway pressure being the primary treatment for mild, moderate, and severe obstructive sleep apnea. 2) It also discusses the importance of weight loss, positional therapy, and lifestyle changes like avoiding alcohol and sedatives as secondary or supplemental treatments. 3) Home sleep testing devices are presented as alternatives to in-lab polysomnography for diagnosing sleep apnea, with minimum requirements for measuring airflow, respiratory effort, and blood oxygenation.























































































