Quintaliani alterazioni metaboliche
•
2 likes•702 views

Alterazioni metaboliche nella IRC Agire prima che sia troppo tardi

Recommended
Recommended
More Related Content
What's hot
What's hot (9)
Similar to Quintaliani alterazioni metaboliche
Similar to Quintaliani alterazioni metaboliche (20)
More from Giuseppe Quintaliani
More from Giuseppe Quintaliani (20)
Quintaliani alterazioni metaboliche
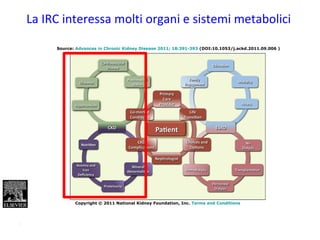
- 1. Source: Advances in Chronic Kidney Disease 2011; 18:391-393 (DOI:10.1053/j.ackd.2011.09.006 ) Copyright © 2011 National Kidney Foundation, Inc. Terms and Conditions La IRC interessa molti organi e sistemi metabolici 1
- 2. SINDROME UREMICA ALTERAZIONI > METABOLICHE E NUTRIZIONALI > ENDOCRINE > IDROELETTROLITICHE > CARDIOCIRCOLATORIE > OSSEE > NEUROLOGICHE 2
- 3. early! late! too late! 3 Ma quando iniziano le alterazioni metaboliche?
- 4. Interpretation eGFR less than 60 mL/min/1·73 m2 and ACR 1·1 mg/mmol (10 mg/g) or more are independent predictors of mortality risk in the general population. This study provides quantitative data for use of both kidney measures for risk assessment and definition and staging of chronic kidney disease
- 5. Meta-analyses in GP, high-risk and CKD cohorts (N=1.5 M) — macroalbuminuria — microalbuminuria — no albuminuria Albuminuria: Marcatore principale di rischio CV e renale Levey, KDIGO, KI 2011Levey, KDIGO, KI 2011
- 6. 6
- 7. •In conclusion, in a large, nationally representative sample of US adults, reduced eGFR was associated with a higher prevalence of anemia, acidosis, hyperphosphatemia, hyperparathyroidism, and hypertension at all ages, even among participants 80 years of age. These findings suggest that clinical evaluation of concurrent CKD complications should be considered for all patients with reduced eGFR, regardless of age 7
- 9. 9
- 10. Triade Scompenso Cardiaco- Insufficienza renale-Anemia Mortalità annua per tutte le cause
- 11. Normal Ca2+ Ca2+ PO4 3– ReleaseBone Kidneys Ca2+ reabsorption PO4 3– excretion PTH Metabolismo minerale Normale Brown EM. In: The Parathyroids – Basic and Clinical Concepts 2nd ed. 2001. Bilezikian JP et al. (eds) PTH, parathyroid hormone Ca2+ Parathyroid glands Calcitriol 11 IL FOSFORO
- 12. fosforo sierico Rischiorelativodimorte 0 0,4 0,8 1,2 1,6 2,0 2,4 2,8 < 2,5 2,5-2,99 3,0-3,49 3,5-3,99 4,0-4,49 4,5-4,99 >5,0 Rischio relativo di morte per livelli di fosforo nei pazienti con IRC n=3.490 Pazienti con IRC from: Kestenbaum B, J Am Soc Nephrol 16:520-528 2005 12
- 13. Geoffrey A. Block, J Am Soc Nephrol 2004; 15: 2208-2218 Elevated serum phosphorus increases mortality risk 13
- 14. Fosforemia mg/dL RischioCVD Nella popolazione generale, senza CVD or CKD, all’aumentare della fosforemia, aumenta il rischio CV 0,4 0,6 0,8 1,0 1,2 1,4 1,6 00 2,6 2,8 3,0 3,2 3,4 3,6 3,8 Dhingra R. et al. Arch Intern Med 2007;167:879 • 3369 soggetti • 16 anni follow-up • +1 mg P = RR 31% • = NO Uprot. e GFR > 90 Fosforemia e rischio di morte 14
- 15. 15 Boaz M, J Am Diet Assoc 1996per la restrizione di Fosforo è necessaria la restrizione di Proteine Rapporto proteine Fosforo 13 mg di P ogni gr di proteine
- 16. • potassio: fino a che il filtrato glomerulare si mantiene intorno ai 20 ml/nim non si verifica in genere iperpotassiemia, anche perchè la ridotta escrezione renale è compensata da un aumento dell’escrezione fecale. Particolare attenzione va posta in corso di malattie catabolizzanti e/o in dialisi. Una iperpotassiemia è estremamante pericolosa : si può arrivare al blocco cardiaco senza che il paziente avverta particolari sintomi. Principali problemi metabolici in corso di IRC POTASSIO 16
- 17. Iperpotassiemia • Ace inibitori o ARB • farmaci risparmiatori • ipoaldosteronismo Sale farmacia “Novosal” -Necrosi cellulare -acidosi -ipoinsulinemia 17
- 18. Quintaliani18 IL SALE Fonti: • sale da cucina, • alimenti preconfezionati Il sale è in relazione alla SETEsoprattutto in dialisi!!!
- 19. • Conclusions A modest reduction in salt intake causes significant and, from a population viewpoint, important falls in blood pressure in both hypertensive and normotensive individuals, irrespective of sex and ethnic group. • The current recommendations to reduce salt intake from 9-12 to 5-6 g/day will have a major effect on blood pressure, but a further reduction to 3 g/day will have a greater effect and should become the long term target for population salt intake. Aprile 2013
- 20. Acidosi e Catabolismo Ossidazione AA (uMol/kg/h) P<0.01 P<0.01 Catabolismo Proteico (uMol/kg/h) Plasma HCO3 (mM) 15 21 1415 21 14 P<0.05 P<0.0 1 0 10 20 50 90 130 from: Reaich et al. Am J Physiol, 1993 20
- 21. Acidosi e metabolismo proteico bilanciofenilalanina nmol/min 16 18 20 22 24 HCO3 10 18 26 30 r = -0.77; p<0.02 from: Garibotto et al. Kidney Int 1994; 45:1432 21 Una dieta di tipo “occidentale” produce all’ incirca 1 mmoL / kg peso corporeo (BW) / die di acidi non carbonici Che derivano prevalentemente dal metabolismo di aminoacidi solforati e cationici e dall’ idrolisi dei fosfati introdotti con la dieta
- 22. Source: American Journal of Kidney Diseases 2013; 62:670-678 (DOI:10.1053/j.ajkd.2013.01.017 ) Copyright © 2013 National Kidney Foundation, Inc. Terms and Conditions Association of Serum Bicarbonate With Risk of Renal and Cardiovascular Outcomes in CKD: A Report From the Chronic Renal Insufficiency Cohort (CRIC) Study Mirela Dobre, MD, MPH, Wei Yang, PhD, Jing Chen, MD, MSc, Paul Drawz, MD, MHS, L. Lee Hamm, MD, Edward Horwitz, MD, Thomas Hostetter, MD, Bernard Jaar, MD, Claudia M. Lora, MD, Lisa Nessel, MSS, MLSP, Akinlolu Ojo, MD, PhD, MPH, Julia Scialla, MD, MHS, Susan Steigerwalt, MD, Valerie Teal, MS, Myles Wolf, MD, MMSc, Mahboob Rahman, MD, MS and CRIC Investigators
- 23. 23 Motivi per i quali si effettua un trattamento dietetico in nefrologia 1. Ridurre le alterazioni metaboliche e la sintomatologia “STATO UREMICO” 2. Ridurre il rischio clinico 3. Ritardare la progressione 4. Impedire la Malnutrizione
- 24. Cardiovascular Mortality in the General Population and in ESRD Treated by DialysisCardiovascular Mortality in the General Population and in ESRD Treated by Dialysis 0.01 100 10 1 0.1 Annual mortality (%) 25–34 45–54 65–74 ≥8535–44 55–64 75–84 Male Female Black White Dialysis General population Age (years) 24
- 25. Chronic Kidney Disease TChronic Kidney Disease Tipping the Scale to the Benefit of Angiotensin-Converting Enzymeipping the Scale to the Benefit of Angiotensin-Converting Enzyme Inhibitors in Patients With Coronary Artery DiseaseInhibitors in Patients With Coronary Artery Disease McCullough PA, Circulation. 2006;114:6-7Chronic Kidney Disease CKD Coronary Artery DiseaseCoronary Artery Disease CAD Combined CKD & CAD Screening ““Intersection between patients with CKD andIntersection between patients with CKD and patients with CVD shows that approximately halfpatients with CVD shows that approximately half of patients with CKD have CAD,of patients with CKD have CAD, whereas 20% ofwhereas 20% of those with CAD will meet a definition of CKDthose with CAD will meet a definition of CKD”” 25
- 26. 26
- 27. Quintaliani Rates of Death at Three Years from Cardiovascular Causes According to the Estimated GFR in Post-MI Adults Anavekar NS et VALIANT Study Group Follow Up: 24.7 months Patients with Cr >2.5 mg/dl excluded 27Relation between Renal Dysfunction and Cardiovascular Outcomes after Myocardial Infarction
- 28. Quintaliani 28 A low-nitrogen diet with protein of high biological value for severe chronic uremia. Giovannetti S, Maggiore Q: Lancet I:1100:1004,1964 28
- 29. Quintaliani Suggerimenti di pratica clinica SIN • Sebbene una TDN a tenore proteico ridotto abbia un’efficacia limitata nel rallentamento della progressione dell’IRC così come valutabile dalla velocità di filtrazione glomerulare, è ben evidente la rilevanza individuale e sociale della dimostrata efficacia nella riduzione della morte renale. In assenza di prove definitive di efficacia, una TDN dovrebbe essere iniziata per lo meno in presenza delle alterazioni metaboliche dell’IRC e senz’altro a valori di filtrato <45 mL/min/m2 29
- 30. 30 Motivi per i quali si effettua un trattamento dietetico in nefrologia 1. Ridurre la sintomatologia “STATO UREMICO” 2. Ridurre il rischio clinico 3. Ritardare la progressione 4. Impedire la Malnutrizione
- 31. Quintaliani31 31
- 32. Quintaliani32 Cap 2 C :Motivi per i quali si effettua un trattamento dietetico in nefrologia: Impedire la Malnutrizione 32
- 33. Malnutrizione- Infiamamzione Aterosclerosi Paradosso dei fattori di rischio Malnutrizione Proteico Calorica Microinfiamamzione Ridotto intake di nutrienti Perdita di nutrienti con la dialisi Disordini endocrini Comorbidita Acidosi. tossine Ridotta clearance delle cotokine infiammatorie Stress ossidativo Dialisi Ipervolemia - Tossine Anoressia Ipercatabolismo Mortalita’ Ospedalizzazione’ Qualita’ di vita Resistenza all’EPO aterosclerosi cachessia < IMC < Colesterolo Ipoalbuminemia Kalantar-Zadeh K, Ikizler A, Block G, et al. Malnutrition-inflammation complex syndrome in dialysis patients: Causes and consequences. Am J Kidney Dis 2003;42:864-881 Malnutrizione, Infiammazione, Aterosclerosi (MIA)
- 35. Most of these studies suggest that the revised estimates of protein needs, with an average protein requirement of 0.34 gm/kg body weight and that 0.45gm of fully utilized protein/kg will cover the needs of 98% of adults in a population 35
- 36. Energy intake and protein requirements The N balance of adult subject on an adequate intake of protein is sensitive to variations in energy intake, whether from carbohydrate, fat or ethanol This means that N balance will be the resultant of the level of energy fed as well as the protein level. This emphasizes the need to define protein requirements in relation to caloric intake. In renal failure the caloric intake to obtain nitrogen balance is 35 Kcal/kg IBW 36
- 37. 37 L’uso di prodotti ipoproteici non solo riduce la quantità di fosforo dietetico ma aumenta il rapporto energia/fosforo. La tabella mostra che il rapporto energia/fosforo passa da 1.88 con la pasta comune a 8.55 con quella ipoproteica (significa che posso somministrare una quota energetica circa 8 volte maggiore a parità di fosforo introdotto per quell’alimento). Così avviene per il pane (da 0.94 a 1.15) per i biscotti (da 1.09 a 11.2) e per il latte (da 0.52 a 29.1). Fornire energia non è certo un compito facile (mission impossible?)
Editor's Notes
- Qui si vede come l’albuminuria è un fattore di rischio renal ma anche cardiovascolare e di mortalita’ in generale e quindi andrebbe vista interecettata e trattata
- Unadjusted event rates by quartile of serum bicarbonate (mEq/L). Abbreviations: CHF, congestive heart failure; MI, myocardial infarction; PAD, peripheral artery disease.
- Intersection between patients with CKD and patients with CVD shows that approximately half of patients with CKD have CAD, whereas 20% of those with CAD will meet a definition of CKD. Those with combined CKD and CAD have been shown to have the benefits of RAAS blockade, as shown. RAAS indicates renin-angiotensin-aldosterone system; CKD, chronic kidney disease; CAD, coronary artery disease; ESRD, end-stage renal disease.