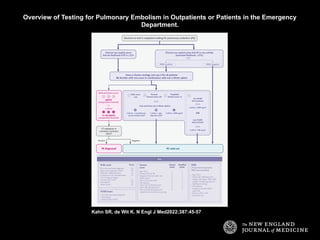
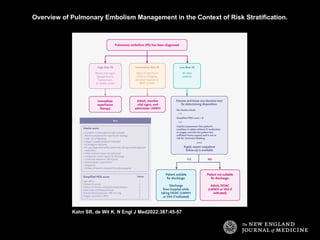
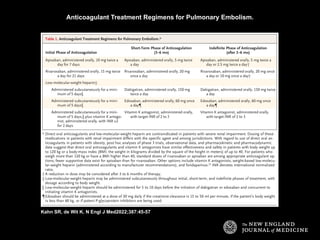
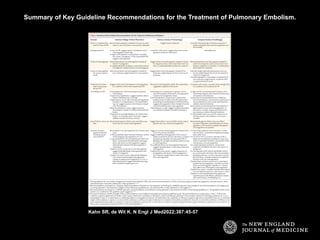
The document discusses a case of a 41-year-old man with breathlessness and a 15% likelihood of pulmonary embolism as assessed by the physician. It recommends d-dimer testing followed by a CT scan to confirm the diagnosis and suggests initiating treatment with a direct oral anticoagulant if embolism is confirmed. Additionally, it advocates for cancer screening based on personal risk and outlines a transition to low-dose anticoagulant therapy after 3 to 6 months, considering the patient's individual preferences.