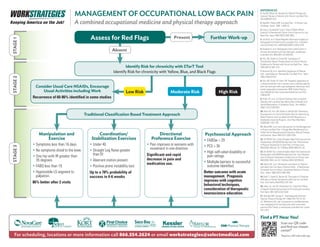
1. Coordination/
Stabilization Exercises
• Under 40.
• Straight Leg Raise greater
than 91.
• Aberrant motion present.
• Positive prone instability test.
Up to a 78% probability of
success in 4-6 weeks
Directional
Preference Exercise
• Pain improves or worsens with
movement in one direction.
Significant and rapid
decrease in pain and
medication use.
Manipulation and
Exercise
• Symptoms less than 16 days.
• No symptoms distal to the knee.
• One hip with IR greater than
35 degrees.
• FABQ less than 19.
• Hypomobile LS segment to
palpation.
86% better after 2 visits
Consider Usual Care NSAIDs, Encourage
Usual Activities including Work
Recurrence of 60-86% identified in some studies
MANAGEMENT OF OCCUPATIONAL LOW BACK PAIN
A combined occupational medicine and physical therapy approach
Further Work-up
For scheduling, locations or more information call 866.554.2624 or email workstrategies@selectmedical.com
REFERENCES
1. AureOF, NilsenJH, VasseljenO. Manual Therapy and
Exercise Therapy in Patients with Chronic Low Back Pain.
Spine28(6)525-532.
2. DeyoRA, Phillips WR. Low Back Pain. A Primary Care
Challenge. Spine. 1996: 1:2826-32.
3. Long A, DonelsonR, Fung T. Does It Matter Which
Exercise? A Randomized Control Trial of Exercise for Low
Back Pain. Spine 2004;29(23):2593-2602.
4. JarvikJG, et al. Rapid Magnetic Resonance Imaging vs.
Radiographs for Patients with Low Back Pain. A Random-
ized Controlled Trial. JAMA2003;289(21):2810-2818.
5. Kendrick D, et al. Radiograph of the Lumbar Spine in
primary care patients with low back pain: randomized
controlled trial. BMJ2001;322:400-405.
6. Fritz JM, Delitto A, Erhard RE. Comparison of
Classification-Based Therapy Based on Clinical Practice
Guidelines for Patients with Acute Low Back Pain. Spine
2003;28(13):1363-1372.
7. Brennan GP, et al. Identifying Subgroups of Patients
with cute/Subacute “Nonspecific”Low Back Pain. Spine
2006;31(6):623-631.
8. Fritz JM, Childs JD, Flynn TW. Pragmatic application of
a clinical prediction rule in primary care to identify patients
with low back pain with a good prognosis following a brief
spinal manipulation intervention. BMC Family Practice.
July 2005,(6):29. http://www.biomedcentral.com/1472-
2296/6/29)
9. Childs JD, et al. A Clinical Prediction Rule to Identify
Patients with Low Back Pain Most Likely to Benefit from
Spinal Manipulation: A Validation Study. Ann IntMed.
2004; 141(12):920-928.
10. Hicks GE, Fritz JM, Delitto A, McGill SM. Preliminary
Development of a Clinical Prediction Rule for Determining
Which Patients with Low Back Pain Will Respond to a
Stabilization Exercise Program. Arch Phys Med Reha-
bil2005;86:1753-1762.
11. Wand BM, et al. Early Intervention for the Management
of Acute Low Back Pain. A Single-Blind Randomized Con-
trolled Trial of Biopsychosocial Education, Manual Therapy,
and Exercise. Spine 2004;2(21):2350-2356.
12. UK BEAM Trial. United Kingdom Back Pain Exercise and
Manipulation (UK BEAM) Randomized Trial: Effectiveness
of Physical Treatments for Back Pain in Primary Care.
BMJ2004. BMJ,dio:10.1136/bmj.38282.6692225. AE
13. UK BEAM Trial. United Kingdom Back Pain Exercise and
Manipulation (UK BEAM) Randomized Trial: Cost Effective-
ness of Physical Treatments for Back Pain in Primary Care.
BMJ2004. BMJ, doi:10.1136/bmj.38282.607859.AE.
14. Burton AK, et al. Information and Advice to Patients
with Back Pain Can Have a Positive Effect. A Randomized
Controlled Trial of a Novel Educational Booklet in Primary
Care. Spine 1999;24(23):2484-2491.
15. Bush T, CherkinD, Barlow W. The Impact of Physician
Attitudes on Patient Satisfaction with Care for Low Back
Pain. Arch Family Med1993;2:301-305.
16. Hides JA, Jull GA, Richardson CA. Long-Term Effects
of Specific Stabilizing Exercises for First-Episode Low Back
Pain.Spine 2001;26(1):E243-E248.
17. Nicholas MK, George S. Psychologically Informed
Practice. Physical Therapy 2011;99(5):765-776.18. Hill
JC, Whitehurst DG, etal. Comparison of stratified primary
care management for low back pain with current best
practice (STarT Back): a randomized controlled trial. Lancet
2011;29:3
Find a PT Near You!
Scan our QR code
and find our closest
center!*
*Requires a QR code reader app.
STAGE3STAGE2STAGE1
Present
Psychosocial Approach
• FABQw 29
• PCS 30
• High self-rated disability or
pain ratings.
• Multiple barriers to successful
outcome identified.
Better outcome with acute
management. Prognosis
improves with cognitive
behavioral techniques,
consideration of therapeutic
neuroscience education.
High RiskLow Risk
Traditional Classification Based Treatment Approach
Identify Risk for chronicity with STarT Tool
Identify Risk for chronicity with Yellow, Blue, and Black Flags
Moderate Risk
Assess for Red Flags
Absent