Download to read offline




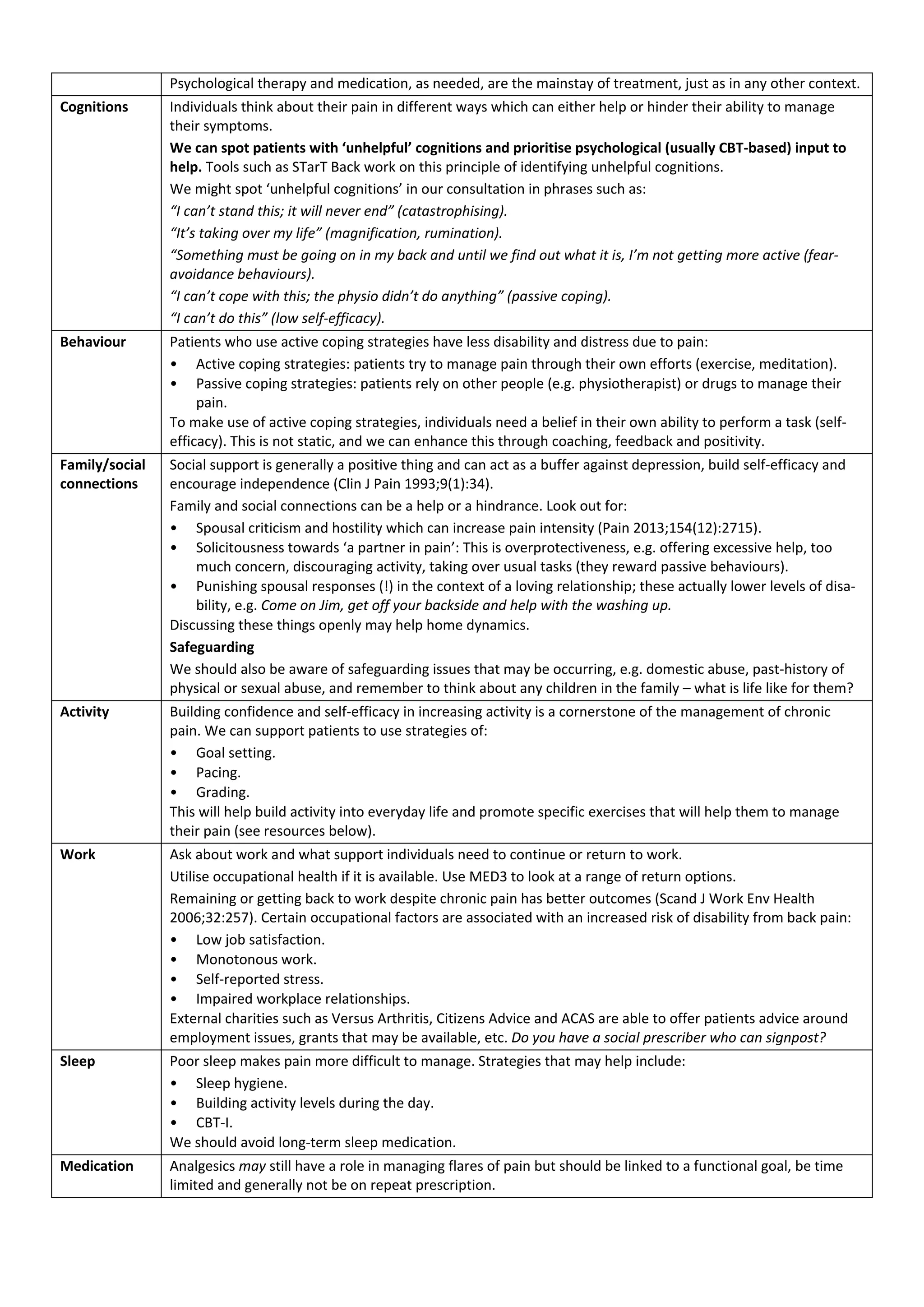
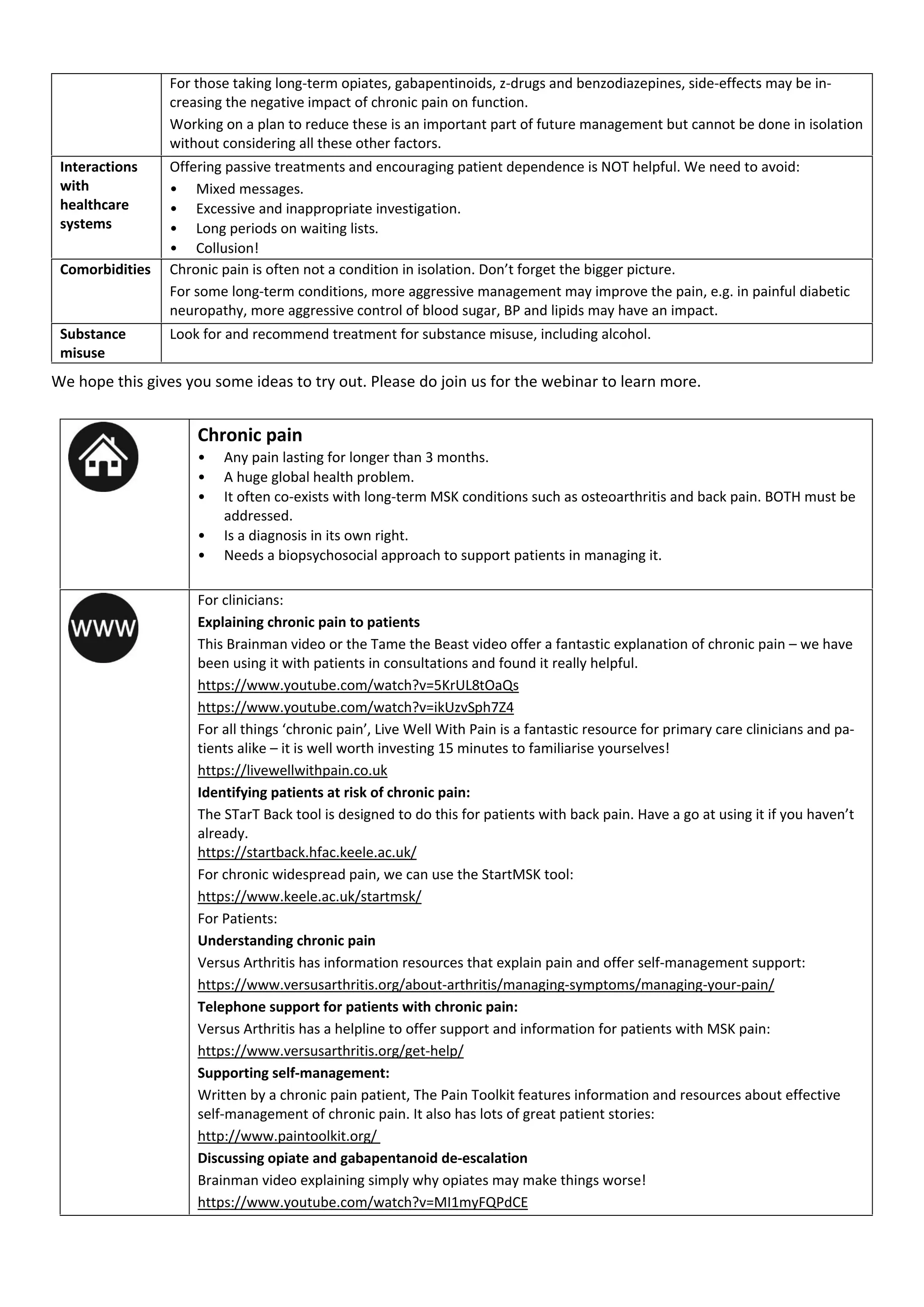



Chronic pain affects a significant portion of the global population, often leading to substantial distress, disability, and feelings of abandonment, particularly due to the opioid crisis and lack of resources. Unlike acute pain, chronic pain is often maladaptive, influenced by neurobiological, psychological, and behavioral factors, necessitating a holistic biopsychosocial approach to management rather than a focus on finding a cure. This document emphasizes the importance of self-management strategies, clear communication with patients, and the integration of psychological support to improve outcomes for individuals suffering from chronic pain.























































































