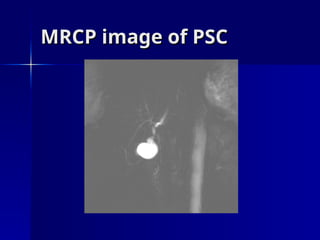
Primary sclerosing cholangitis (PSC) is a chronic inflammatory cholestatic disease characterized by the progressive destruction of bile ducts, often associated with inflammatory bowel disease, particularly ulcerative colitis. The condition has a male predominance and can present asymptomatically, with symptoms developing over time including jaundice and fatigue, and carries a lifetime risk of cholangiocarcinoma and other cancers. Management primarily involves liver transplantation as the only treatment shown to improve survival, while other medical therapies display inconsistent results.


























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










