Download as PDF, PPTX

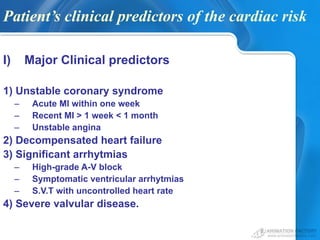


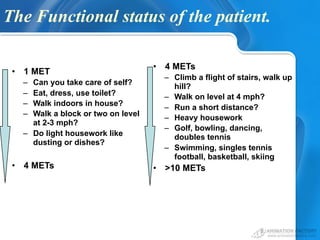
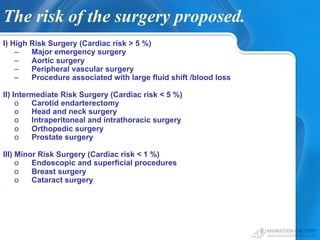

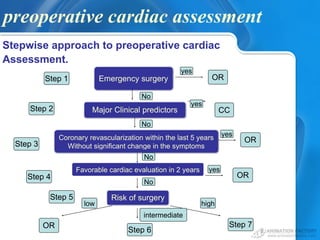
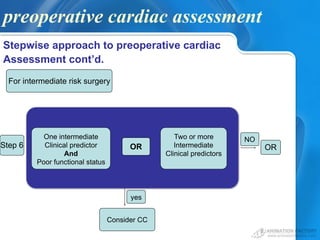
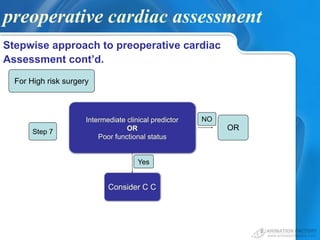




This document discusses preoperative cardiac assessment for surgery. It begins by outlining why cardiac assessment is needed before surgery to determine a patient's risk and medical management needs. It then describes the questions that should be considered in the assessment, including the urgency of surgery, recency of cardiac evaluation, patient risk factors, functional status, and risk of the planned surgery. The document provides guidelines for collecting preoperative data through a stepwise assessment process and discusses when cardiac consultation may be needed. It concludes by noting new concepts in assessment and that for elective surgery, it is reasonable to wait 4-6 weeks after a myocardial infarction before proceeding.