The document summarizes pregnancy diagnosis and the physiological changes that occur during pregnancy. It discusses how pregnancy is diagnosed through hormone detection in urine or blood tests. It then outlines the signs and symptoms of each trimester of pregnancy. Finally, it describes the maternal anatomical and physiological changes that occur in the reproductive, cardiovascular, and respiratory systems to accommodate the growing fetus.

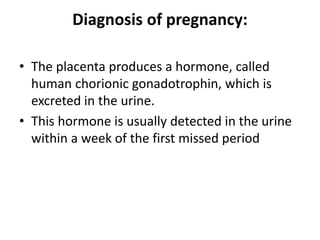
![Reproductive organs:
• Body of the uterus: There is an increase in
growth and enlargement of the body of the
uterus.
• The muscle fibres undergo both hypertrophy
and hyperplasia [both increase in length and
breath and addition of new muscle fibres.]
• The uterus feels soft and elastic in contrast to
firm feel of the nongravid uterus.](https://image.slidesharecdn.com/pregnancyphysiologyandadaptation-231011231102-80ea239b/85/pregnancy-physiology-and-adaptation-ppt-23-320.jpg)

















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




