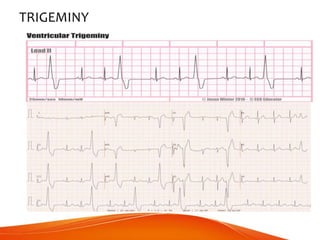
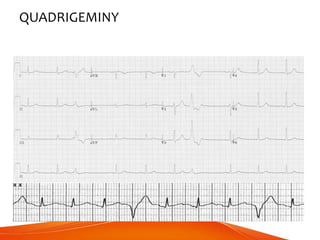
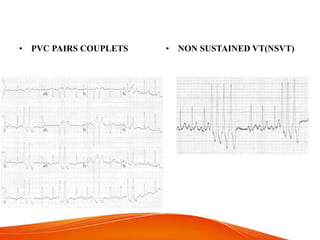
This document discusses premature ventricular contractions (PVCs), which are extra heartbeats originating from the ventricles that disrupt normal heart rhythm. PVCs are common and usually harmless, but may require treatment if frequent or in those with heart disease. The document covers causes of PVCs including caffeine and stress, different types classified by origin and pattern, characteristics that indicate worse prognosis, and potential complications if left untreated, such as cardiomyopathy or cardiac arrest.