Eligible couple: Currentlymarried couple and female is in reproductive
age group.
Target couple: who has completed family and has at least one live
child. Targets for permanent sterilization.
4.
Pearl index
• Itis the measure of the safety of contraceptives. The smaller the pearl index, the
safer the method of contraception.
• If 5 pregnancies occur among 120 women using a contraceptive method over a
period of 12 months, the Pearl Index would be calculated as follows:
• This means there are 4.17 pregnancies per 100 women per year for this
contraceptive method.
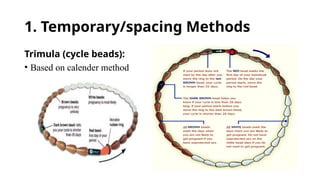
Barrier methods
The aimof barrier method is to prevent live sperm from meeting ovum.
Provide some protection against STDs.
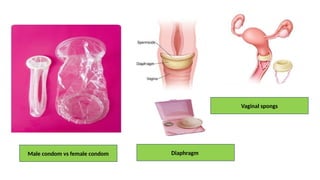
• Nirodh (male condom), fem. Condom, diaphragm (dutch cup), vaginal
sponge (Today)
• S/E: hypersensitivity
Chemical methods
• Foam, cream, suppositories, , soluble films.
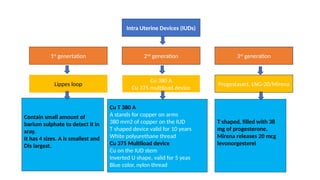
Intra Uterine Devices(IUDs)
1st
genertation 2nd
generation 3rd
generation
Lippes loop
Cu 380 A
Cu 375 multiload device
Progestasert, LNG-20/Mirena
Cu T 380 A
A stands for copper on arms
380 mm2 of copper on the IUD
T shaped device valid for 10 years
White polyurethane thread
Cu 375 Multiload device
Cu on the IUD stem
Inverted U shape, valid for 5 yeas
Blue color, nylon thread
T shaped, filled with 38
mg of progesterone.
Mirena releases 20 mcg
levonorgesterel
Contain small amount of
barium sulphate to detect it in
xray.
It has 4 sizes. A is smallest and
Dis largest.
9.
Intra Uterine Devices
•MOA: Impair fertilization and implantation
• S/E: Bleeding, pain, PID, perforation
Timing of insertion
• During menstruation or within 10 days of the menstruation.
• Can be inserted within 48 hours of delivering or after 6 weeks of delivery.
• Ectopic pregnancy is not a contraindication.
• Inserted up till 5 days of unprotected intercourse.
• Within 10 minutes of placenta removal.
10.
Hormonal methods
1. CombinedOral Contraceptive pills:
Contain low doses of synthetic hormones progestin and estrogen.
• Ethinyl estradiol 0.03 mg + levonorgestrel 0.15mg
• MALA N: free supply
• MALA-D social marketing on payment 3 rupees per packet.
11.
COCPs:
• MOA: interruptovulation
• Side effects:
• metabolic- DM, dyslipidemia, weight gain,
• Cardiac: thrombotic, CAD, stroke, raised liver enzyme
• Carcinogenic: promote ca cervix and ca breast
• NOTE: protects ca ovary, ca endometrium, benign breast disease, DUB
• Dose: 21 hormonal pills and 7 iron tablets daily.
• Contraception of choice for delaying 1st
child.
• Avoid during breasfeeding.
• Lowest failure rate among contraceptives under the NFPP.
12.
2. Progestin onlypill:
• Contain synthetic hormone progestin in lower doses.
• a/k/a minipill and micropill.
• Safe for breastfeeding women, can be started earlier than 6 weeks.
• Started on the 1st
day of menstruation.
• Start next pack on the very next day of last dose of previous pack.
13.
3. Chhaya/Saheli
• Non-steroidnon-hormonal contraceptive.
• Developed by cdri, Lucknow
• Market name: Centchroman-30 tablets
• Active chemical name: ormiloxifene
• MOA: Prevent the implantation of fertilized ovum.
• S/E: delayed periods
• Dose: 30 mg tablet twice weekly for first three months and then weekly.
• 1st
pill on 1st
day of period, 2nd
pill on 4th
day of period and pattern of taking pill continue.
14.
4. postcoital contraception(emergency contraceptive pill):
• a/k/a morning after pill, iPILL, Ezy pill- levonorgesterel 1.5 mg
• Single dose, started ASAP but < 72 hours of unprotected intercourse
• Another method is mifepristone 10 mg once within 72 hours.
5. Once a month pill:
• Long acting.
• Long acting estrogen (quinestrol)+ short acting progesterone
• High failure rate
6. Male pill:
• Made up of gossypol cotton seed derivative
• Causes oligo or azoospermia
• 10% men become parmenantly azoospermic after taking for 6 months.
15.
Injectable contraceptive:
Antra: DMPA
•Injectable (I/M)
• Medroxy progesterone acetate
• @ 150 mg every three monthly.
• Can be taken 2 weeks early and 4 weeks after the due date for
injection.
16.
PERMANENT METHODS
• Tubectomyand vasectomy
• Mechanical method of inhibiting fertilization
• S/E operation related; infection, pain
• Note; for vasectomy use alternate contraception for 8-9 weeks or 30
ejaculation
17.
• Female Sterilisation
•● Two techniques:
• o Minilap: Minilaparotomy involves making a small incision in the abdomen. The fallopian
tubes are brought to the incision to be cut or blocked. Can be performed by a trained MBBS
doctor.
• o Laparoscopic: Laparoscopy involves inserting a long thin tube with a lens in it into the
abdomen through a small incision. This laparoscope enables the doctor to see and block or
cut the fallopian tubes in the abdomen. Can be done only by trained and certified MBBS
doctor or specialist.
• Male Sterilisation
• Two techniques being used in India: o Conventional
• o Non- Scalpel Vasectomy – no incision, only puncture and hence no stitches
• the couple needs to use an alternative method of contraception for first three months after
sterilization till no sperms are detected in semen.
18.
National family planning
programme
•India was the first country in the world to have launched a National Programme
for Family Planning in 1952.
• Contraceptive services under the Programme
1.Oral Contraceptive Pills (OCPs)
Delivery of OCPs at the doorstep by ASHA. Pills are also available free of cost.
2.Condoms
Free brand ‘Nirodh’ available at government facilities.
3.Intra-Uterine Contraceptive Devices (IUCD)
4.Female sterilisation
5.Male sterilisation
6.Emergency Contraceptive Pill (ECP)