Recommended

More Related Content
What's hot
What's hot (20)
Similar to Poster for comparision of spinal and TAP block in inguinal hernia repaie surgery
Similar to Poster for comparision of spinal and TAP block in inguinal hernia repaie surgery (20)
Recently uploaded
Recently uploaded (20)
Poster for comparision of spinal and TAP block in inguinal hernia repaie surgery
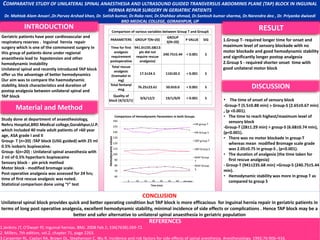
- 1. o CONCLUSION Unilateral spinal block provides quick and better operating condition but TAP block is more efficacious for inguinal hernia repair in geriatric patients in terms of long post operative analgesia, excellent hemodynamic stability, minimal incidence of side effects or complications . Hence TAP block may be a better and safer alternative to unilateral spinal anaesthesia in geriatric population REFERENCES 1.Jenkins JT, O'Dwyer PJ; Inguinal hernias. BMJ. 2008 Feb 2; 336(7638):269-72. 2. Millers, 7th edition, vol.2, chapter 71, page 2263. 3.Carpenter RL, Caplan RA, Brown DL, Stephenson C, Wu R. Incidence and risk factors for side effects of spinal anesthesia. Anesthesiology. 1992;76:906–916. COMPARATIVE STUDY OF UNILATERAL SPINAL ANAESTHESIA AND ULTRASOUND GUIDED TRANSVERSUS ABDOMINIS PLANE (TAP) BLOCK IN INGUINAL HERNIA REPAIR SURGERY IN GERIATRIC PATIENTS Dr. Mahtab Alam Ansari ,Dr.Parvez Arshad khan, Dr. Satish kumar, Dr.Raka rani, Dr.Shahbaz ahmad, Dr.Santosh kumar sharma, Dr.Narendra deo , Dr. Priyanka dwivedi BRD MEDICAL COLLEGE, GORAKHPUR, UP INTRODUCTION Material and Method DISCUSSION RESULT Geriatric patients have poor cardiovascular and respiratory reserves . Inguinal hernia repair surgery which is one of the commonest surgery in this group of patients done under regional anaesthesia lead to hypotension and other hemodynamic instability Unilateral spinal and recently introduced TAP block offer us the advantage of better hemodynamics Our aim was to compare the haemodynamic stability, block characteristics and duration of postop analgesia between unilateral spinal and TAP block Study done at department of anaesthesiology, Nehru Hospital,BRD Medical college,Gorakhpur,U.P. which included 40 male adult patients of >60 year age, ASA grade I and II Group- T (n=20) :TAP block (USG guided) with 25 ml 0.5% isobaric bupivacaine. Group- S(n=20) : Unilateral spinal anaesthesia with 2 ml of 0.5% hyperbaric bupivacaine Sensory block - pin prick method Motor block - modified bromage scale. Post-operative analgesia was assessed for 24 hrs; time of first rescue analgesic was noted. Statistical comparison done using “t” test 1.Group T- required longer time for onset and maximum level of sensory blockade with no motor blockade and good hemodynamic stability and significantly longer postop analgesia 2.Group S - required shorter onset time with good unilateral motor block • The time of onset of sensory block -Group-T (5.5±0.88 min) > Group-S (2.65±0.67 min) , (p <0.001). • The time to reach highest/maximum level of sensory block -Group-T (28±1.29 min) > group-S (6.68±0.74 min), (p<0.001). • There was no motor blockade in group-T whereas mean modified Bromage scale grade was 2.05±0.75 in group-S , (p<0.001). • The duration of analgesia (the time taken for first rescue analgesia) - Group-T (941±235.68 min) >Group-S (240.75±5.44 min). • Hemodynamic stability was more in group T as compared to group S Comparison of various variables between Group T and GroupS PARAMETERS GROUP T(N=20) GROUP S(N=20) P VALUE SIG Time for first analgesic requirement postoperative 941.0±235.68(13 pts did not require rescue analgesia) 240.75±5.44 ˂ 0.001 S Total rescue analgesic (tramadol in mg) 17.5±24.5 110±20.5 ˂ 0.001 S Total fentanyl mcg 76.25±23.61 50.0±0.0 ˂ 0.001 S Quality of block (4/3/2/1) 0/6/12/2 19/1/0/0 ˂ 0.001 S 60 70 80 90 100 110 120 130 140 150 160 Hemodynamicvalues Time (min) Comparison of Hemodynamic Parameters in both Groups HR group T HR Group S SBP group T SBP Group S MAP Group T MAP Group S 5 10 15 20 30 45 60 after surgery
Editor's Notes
- tb