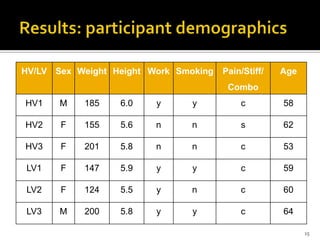
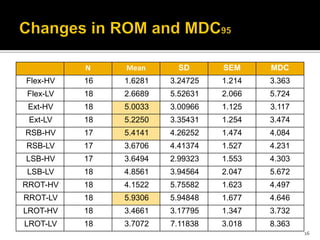
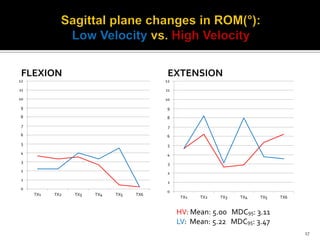
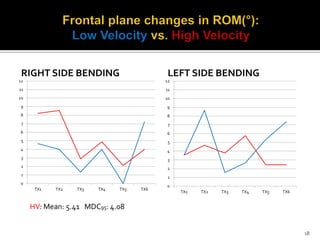
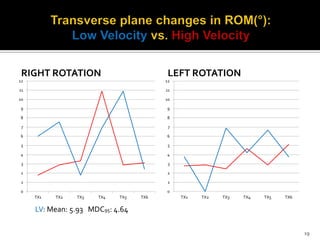
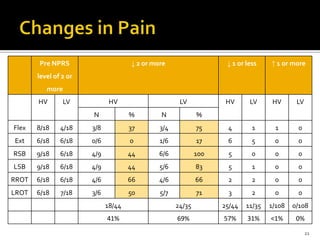
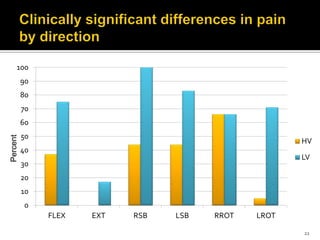
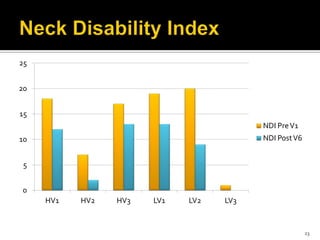
This document describes a preliminary study investigating the effectiveness of Translatoric Spinal Manipulation (TSM) techniques for improving cervical range of motion and pain. The study compared the effects of high velocity (HV) and low velocity (LV) TSM techniques in participants with neck pain and stiffness. The results showed that both HV and LV TSM techniques improved cervical range of motion, reduced pain, and improved function, with no significant differences between the techniques. The LV techniques showed a greater reduction in pain levels compared to HV techniques. No adverse events were reported.