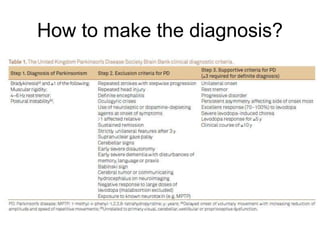
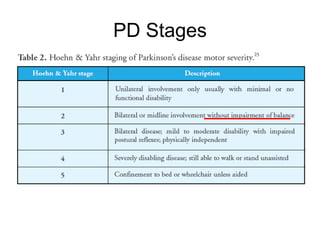
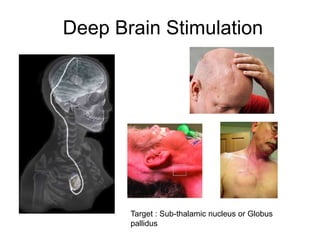
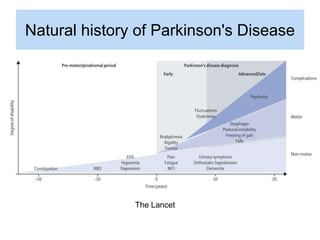
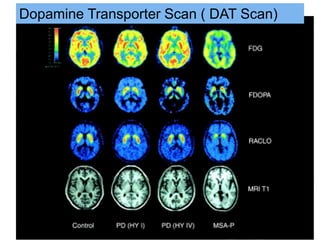
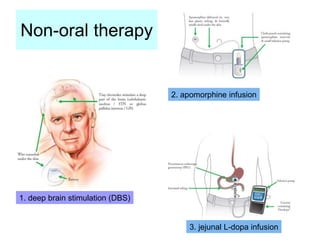
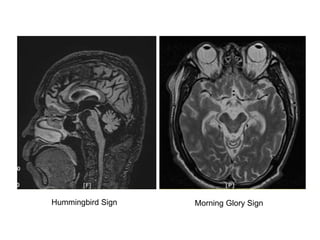
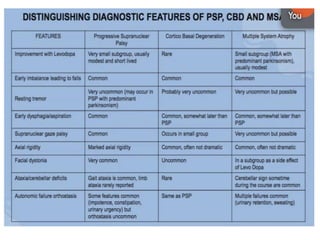
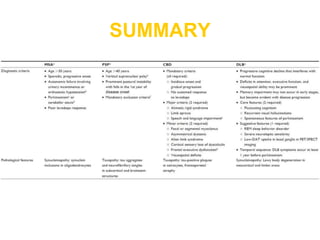
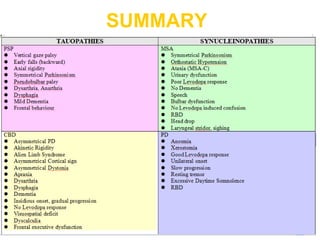
This document summarizes key information about Parkinsonism and related neurological disorders. It provides clinical examination findings for different types of Parkinsonism, including rigidity, tremors, and limb stiffness. It also discusses diagnostic tests such as DAT scans and MRI findings. Deep brain stimulation is mentioned as a treatment for Parkinson's disease. Complications of therapy like levodopa-induced dyskinesia are also summarized. Clinical features of different Parkinson-plus syndromes like MSA, PSP, and CBS are outlined.