Downloaded 552 times




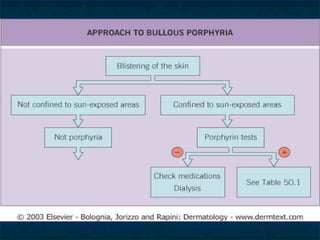




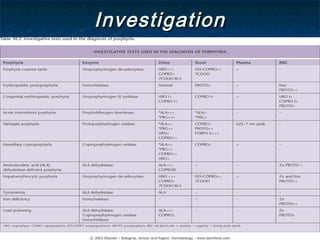



The document summarizes information about Porphyria Cutanea Tarda (PCT), including: - PCT is the most common type of porphyria, caused by a deficiency in the uroporphyrinogen decarboxylase enzyme leading to elevated porphyrin levels. - It is more common in males over 40, and risk factors include alcohol use, iron overload, hepatitis C, and certain medications. - Symptoms include blistering or burning of the skin when exposed to light due to accumulation of water-soluble or lipophilic porphyrins. - Diagnosis involves ruling out other conditions and confirming elevated porphyrin levels bi










































































