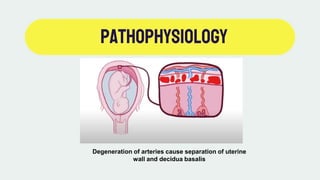
Placenta abruption is the premature separation of the placenta from the uterine wall, which can lead to serious maternal and fetal complications, most commonly occurring after 20 weeks of gestation. Risk factors include trauma, drug use, maternal age, and conditions like hypertension and smoking. Management is critical and may involve emergency cesarean sections, especially in severe cases with hemorrhage and fetal distress.