Downloaded 10 times






























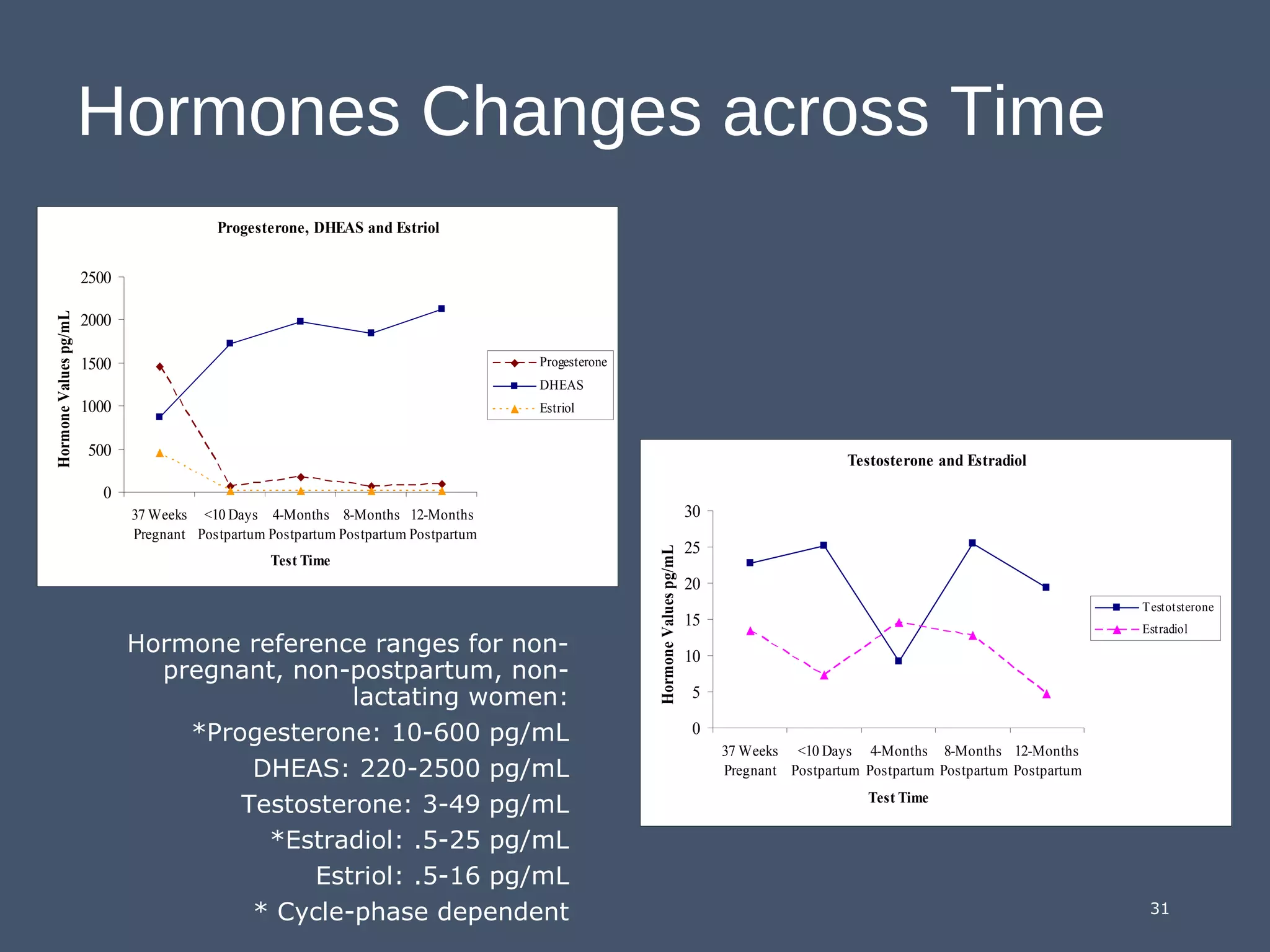







1) The document discusses hormones and their relationship to mood disorders in women, specifically during reproductive stages like puberty, pregnancy, postpartum, and menopause. 2) It presents research showing elevated levels of the adrenal androgen DHEAS are associated with psychiatric symptoms in the postpartum period, while lower levels of pregnancy testosterone may be an early warning sign. 3) The research found that as hormone levels like DHEAS and progesterone normalized in the year following childbirth, psychiatric symptoms tended to abate, though chronically elevated DHEAS was linked to ongoing issues.


![Etoh[1]](https://cdn.slidesharecdn.com/ss_thumbnails/etoh1-140225215207-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)






























































