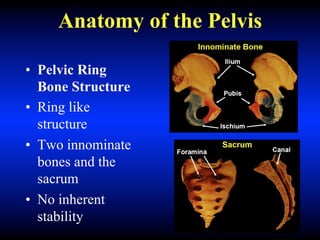
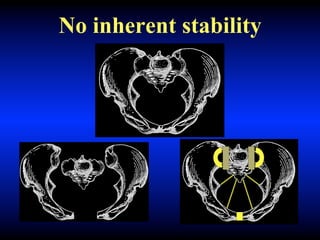
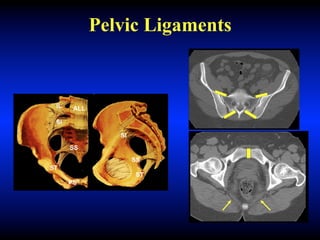
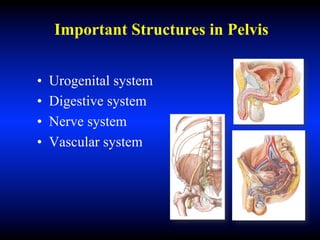
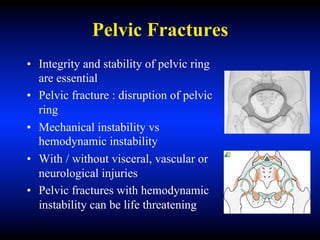
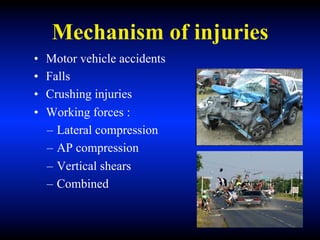
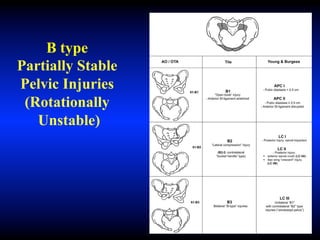
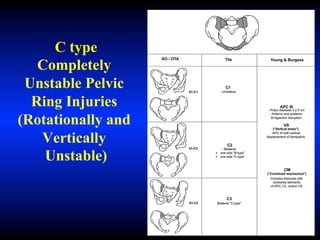
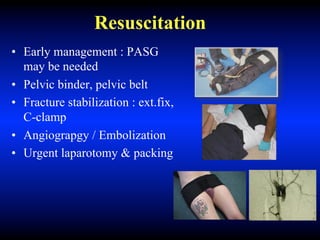
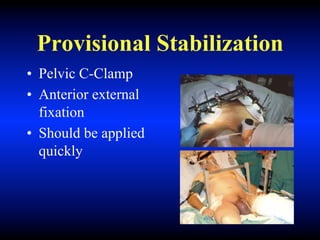
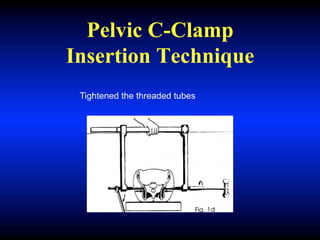
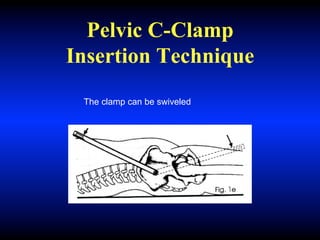
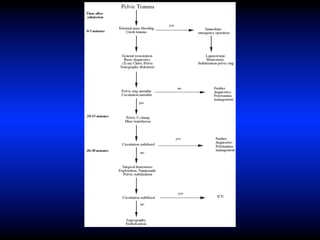
The pelvis has no inherent stability due to its ring-like bone structure connected by ligaments. Pelvic trauma can cause life-threatening bleeding due to proximity to major blood vessels in the highly vascularized bone. Classification systems categorize fractures by stability and force. For unstable fractures with hemorrhage, initial management includes aggressive resuscitation, provisional stabilization techniques like pelvic binding or C-clamps, and potential angiography or surgery to control bleeding. Early recognition and stabilization are crucial for survival in hemodynamically unstable patients with pelvic fractures.