Download as PDF, PPTX
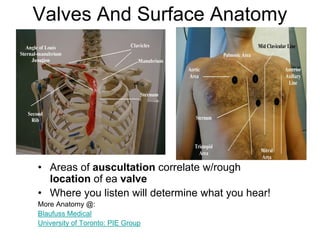
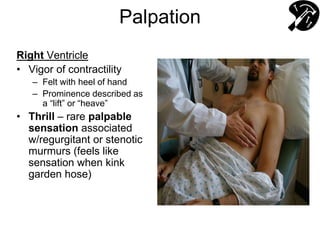
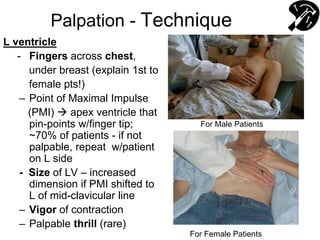
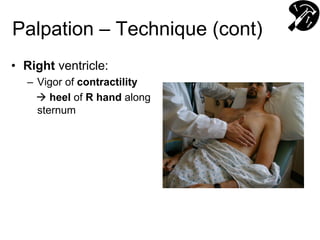
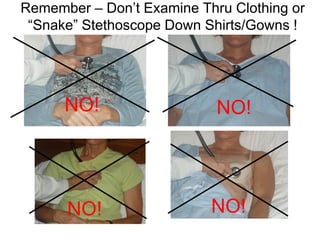
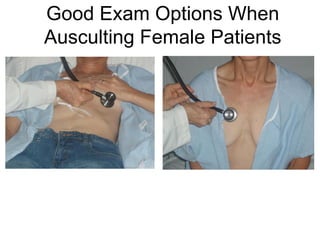
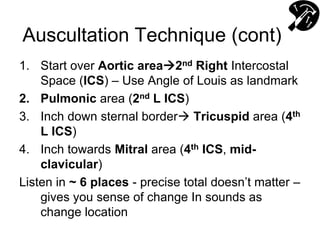
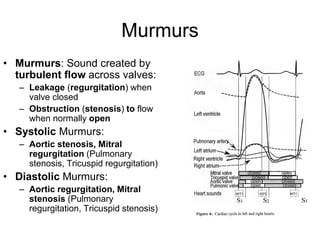
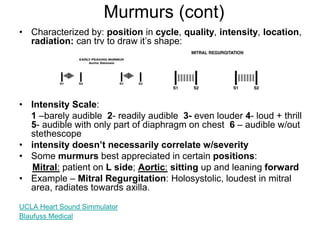
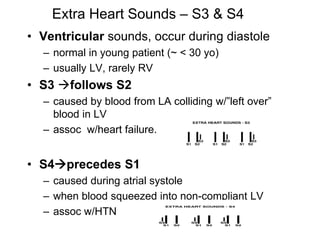
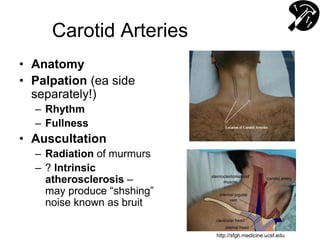
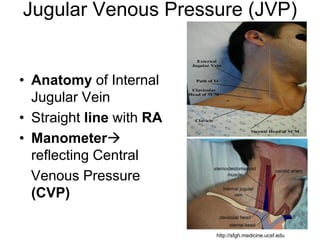
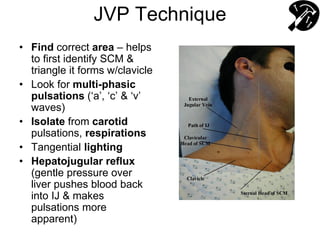
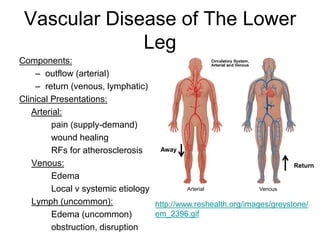
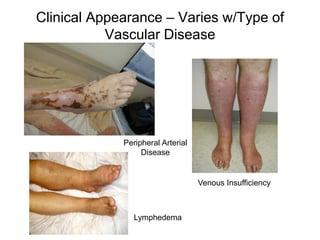
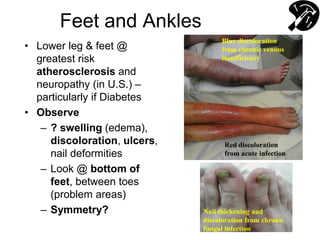
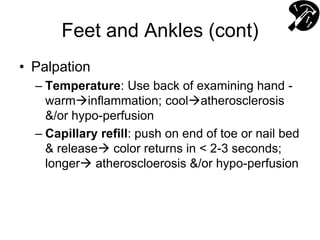
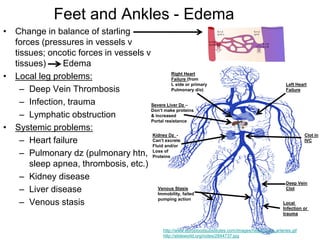
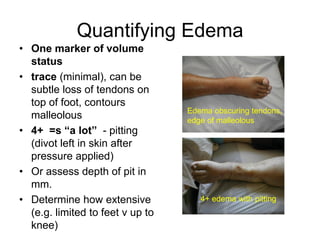
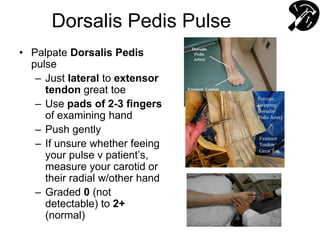
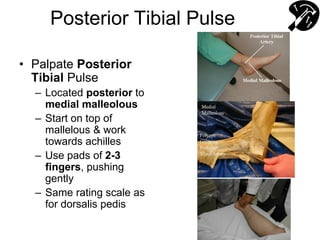

The document provides guidance on performing a cardiovascular exam, including assessing the heart, carotid arteries, jugular veins, and lower extremities. Key steps are listening to heart sounds at multiple locations to identify murmurs or extra sounds, palpating pulses and organs, and examining the legs for signs of vascular disease such as edema, discoloration, or reduced pulses. Proper technique is emphasized, including respectfully draping patients and explaining exam procedures.



















































































