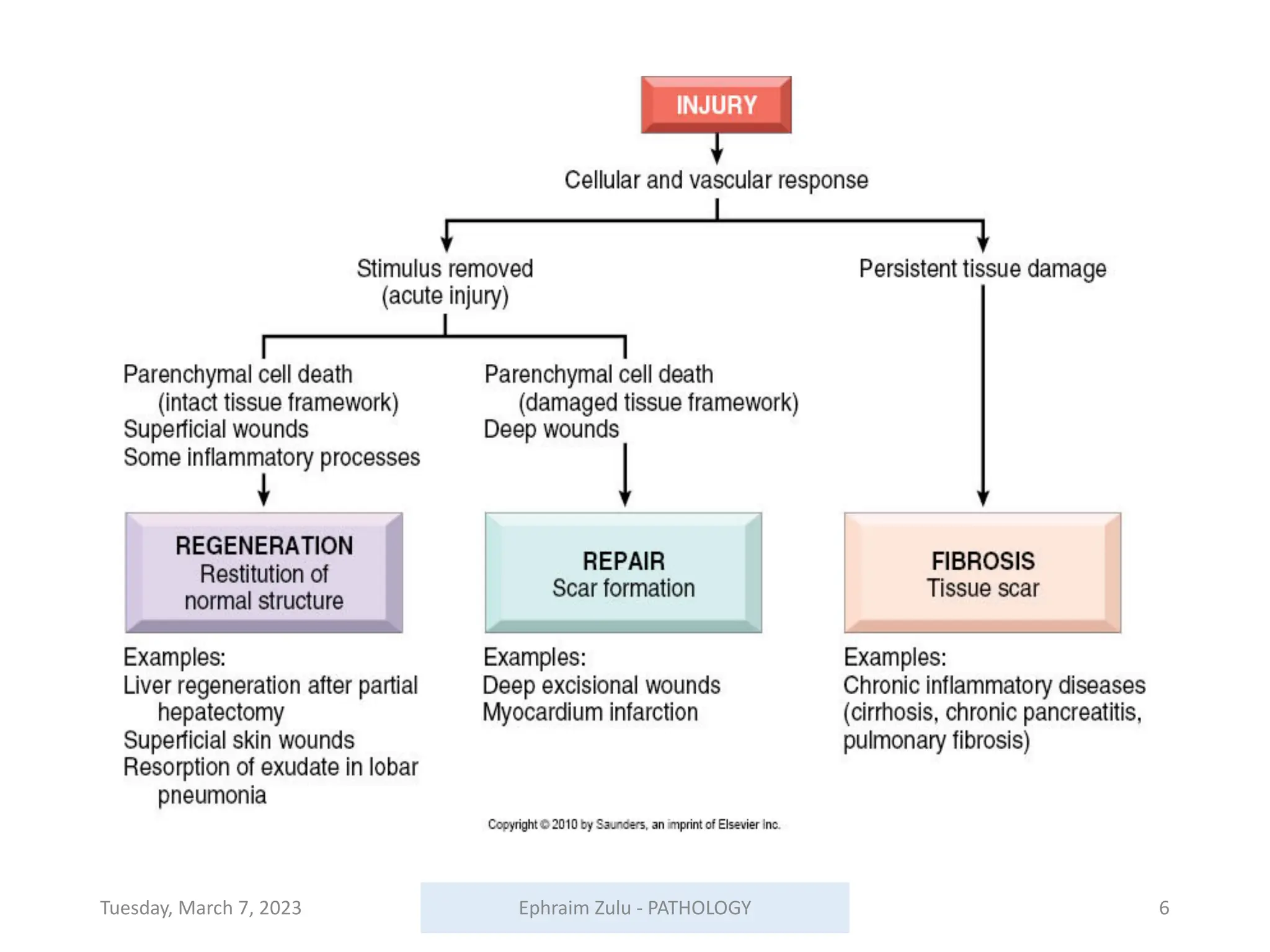
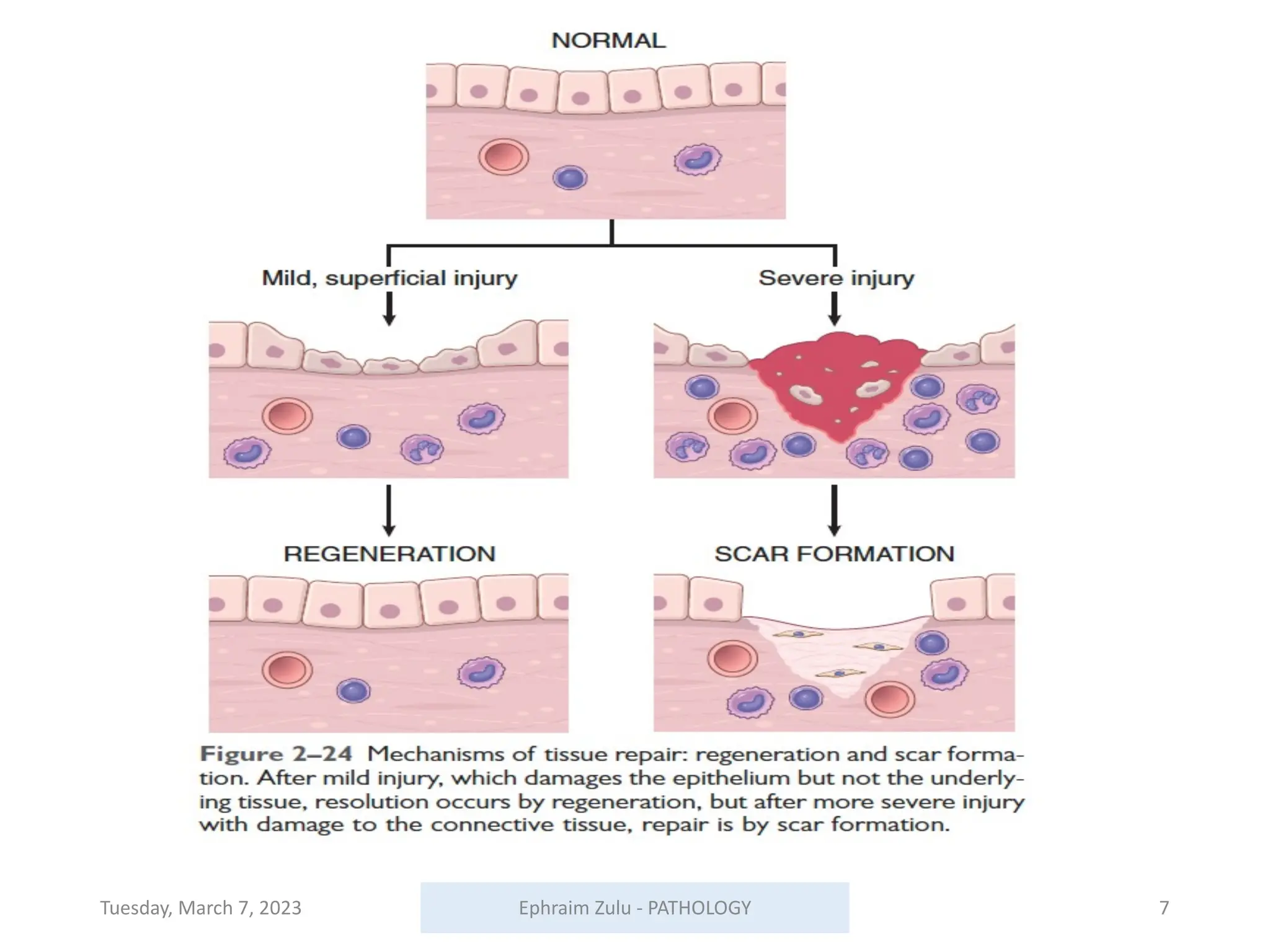
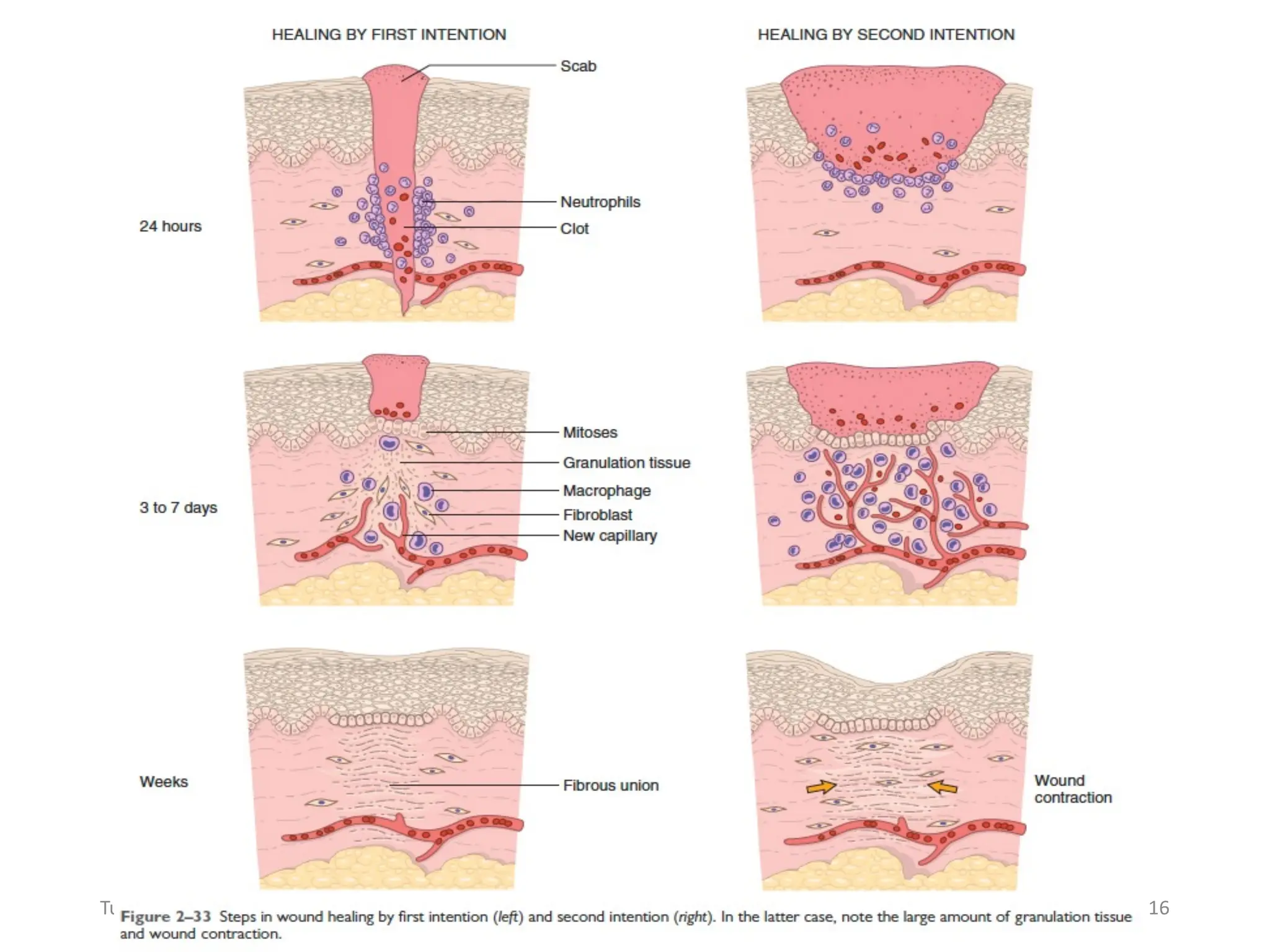
This document outlines a pathology lecture on tissue healing and repair, covering the processes of regeneration and repair, factors influencing wound healing, and complications arising from it. Key learning objectives include understanding different wound healing patterns, the role of various factors, such as infection and nutrition, in healing, and distinguishing between primary and secondary healing. The document also discusses conditions like keloids and hypertrophic scars that can result from abnormal healing.