The document provides an overview of the anatomy of the parotid gland and submandibular gland. It discusses:
- The development of the parotid gland beginning in the 6th week of prenatal development from epithelial buds near the mouth.
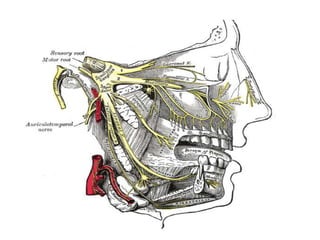
- The location of the parotid gland inferior and anterior to the external acoustic meatus. It drains through the parotid duct into the oral cavity.
- The blood supply and lymphatic drainage of the parotid gland which is mainly from the external carotid artery and to preauricular lymph nodes.
- The submandibular gland develops later than the parotid from buds on the floor of the mouth and grows
























![CT OF SLIVERY GLAND
It is a fatty glandular tissue that is encased in a dense
capsule. Because of this, the parotid gland on CT is
consistently more lucent (-25 to 10 Hounsfield units
[H]) than surrounding muscles (35-60 H) and likewise
is distinctly more radiodense than adjacent fat in the
subcutaneous tissues, infratemponal fossa, and
lateral pharyngeal space(-125 to -50 H)(figs.
1A, 1B, and 2B).](https://image.slidesharecdn.com/parotid-140129162429-phpapp01/85/Parotid-28-320.jpg)






































































































