TEXT
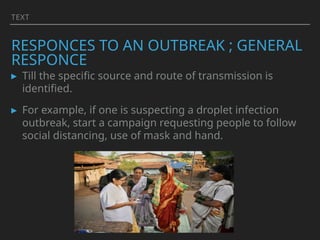
RESPONCES TO ANOUTBREAK ; GENERAL
RESPONCE
▸ Till the specific source and route of transmission is
identified.
▸ For example, if one is suspecting a droplet infection
outbreak, start a campaign requesting people to follow
social distancing, use of mask and hand.
4.
TEXT
RESPONCES TO ANOUTBREAK; SPECIFIC
MEASURES
▸ Depend on causative agent.
▸ BROAD STEPS ARE:
▸ Identification and nullification of the source of outbreak like
chlorinating wells,
▸ Minimising transmission to prevent further exposure: vector
control,
▸ Protection of the host- immunization / chemoprophylaxis,
▸ Controlling the reservoir include early diagnosis, notification,
isolation, treatment, quarantine.
5.
TEXT
▸ Broadly theseare measures, pending results of
epidemiologic/outbreak investigation.
▸ these activities routinely are now included in primary
health care- it requires community participation, political
support and intersectoral co-ordination.
6.
TEXT
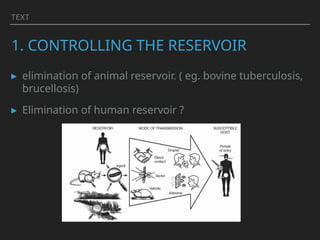
1. CONTROLLING THERESERVOIR
▸ elimination of animal reservoir. ( eg. bovine tuberculosis,
brucellosis)
▸ Elimination of human reservoir ?
7.
1. CONTROLLING THERESERVOIR
STAMPING OUT THE ‘SPARK’ ; (A) EARLY
DIAGNOSIS
▸ the first step in the control of an outbreak is its Rapid
identification.
▸ for treatment of patients;
▸ for epidemiological investigations for eg. the source of
infection from index case (known) to the primary source
(unknown) of infection.
▸ to study tpp —descriptive epidemiology
8.
RESERVOIR
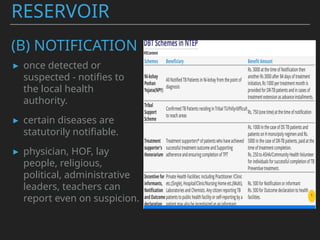
(B) NOTIFICATION
▸ oncedetected or
suspected - notifies to
the local health
authority.
▸ certain diseases are
statutorily notifiable.
▸ physician, HOF, lay
people, religious,
political, administrative
leaders, teachers can
report even on suspicion.
(D) ISOLATION
▸ Oldestds control measure.
▸ “Separation, for the period of communicability of infected
persons or animals from others in such places and under
such conditions, as to prevent or limit the direct or
indirect transmission of the infectious agent from those
infected to those who are susceptible or who may spread
the agent to others”
1. CONTROLLING THE
RESERVOIR
14.
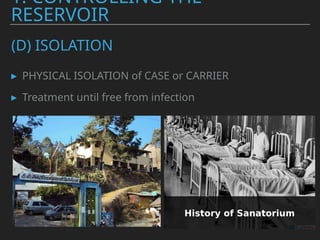
(D) ISOLATION
▸ PHYSICALISOLATION of CASE or CARRIER
▸ Treatment until free from infection
1. CONTROLLING THE
RESERVOIR
15.
(D) ISOLATION
▸ PURPOSE:To protect the community by preventing
transfer of infection from reservoir to the possible
susceptible hosts.
▸ TYPES: varies
▸ Standard isolation, strict isolation, protective, high
security,
▸ Hospital isolation >>>> Home isolation
▸ Difficult in rural areas.
1. CONTROLLING THE
RESERVOIR
16.
(D) ISOLATION
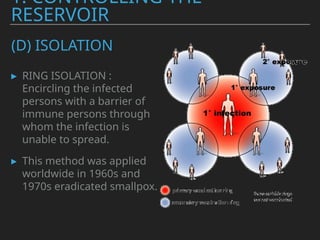
▸ RINGISOLATION : Encircling the infected persons with a
barrier of immune persons through whom the infection
is unable to spread.
▸ Ring isolation in context of Small pox : a public health
strategy where, upon identifying a smallpox case, the
immediate close contacts of that person are isolated and
vaccinated, creating a "ring" of protection around the
infected individual to prevent further spread of the
disease.
1. CONTROLLING THE
RESERVOIR
17.
(D) ISOLATION
▸ RINGISOLATION :
Encircling the infected
persons with a barrier of
immune persons through
whom the infection is
unable to spread.
▸ This method was applied
worldwide in 1960s and
1970s eradicated smallpox.
1. CONTROLLING THE
RESERVOIR
18.
(D) ISOLATION ;WHEN AND FOR WHAT ?
▸ For diseases like Diphtheria, Cholera, Streptococcal
resp disease, pneumonic plague.. Isolation has
distinctive value
▸ However Isolation becomes a futile excercise for ds
where there is a large component of subclincal
infection and carrier state like Polio, Hepatitis A,
Typhoid fever..
▸ Isolation has failed for TB, Leprosy and STDs
1. CONTROLLING THE
RESERVOIR
19.
(D) ISOLATION ;WHEN AND FOR WHAT ?
▸ Isolation has FAILED in the control of ds like Leprosy, TB,
STDs.
▸ here the Concept of Physical isolation has replaced by
CHEMICAL Isolation.
▸ that is rapid treatment of cases in their homes and
rendering them non-infectious as quickly as possible.
▸ in todays times, Isolation is recommended only when the
risk of transmission if the infection is exceptionally
serious.
1. CONTROLLING THE
RESERVOIR
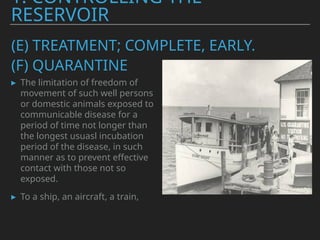
(E) TREATMENT; COMPLETE,EARLY.
▸ The limitation of freedom of
movement of such well persons
or domestic animals exposed to
communicable disease for a
period of time not longer than
the longest usuasl incubation
period of the disease, in such
manner as to prevent effective
contact with those not so
exposed.
▸ To a ship, an aircraft, a train,
1. CONTROLLING THE
RESERVOIR
(F) QUARANTINE
24.
▸ ABSOLUTE QUARANTINE:
▸MODIFIED QUARATINE: A selective partial limitaion of
freedom of movement such as exclusion of children from
school.
▸ SEGRAGATION;
▸ With better techniques of early diagnosis and Rx,
quaratine as a method of disease control has become
outdated.
▸ It has been replaced by Active Surveillance.
1. CONTROLLING THE
RESERVOIR
(F) QUARANTINE
25.
▸ method ofconducting
surveillace.
▸ allows scientist to gather data
about infections and how they
spread.
▸ Once a person tests positive for
a disease, they will be asked to
list the people they have been in
contact with andthe places they
visited during the period in
which they were contagious.
1. CONTROLLING THE
RESERVOIR
(G) CONTACT TRACING:
26.
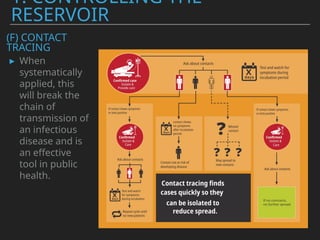
▸ When
systematically
applied, this
willbreak the
chain of
transmission of
an infectious
disease and is
an effective
tool in public
health.
1. CONTROLLING THE
RESERVOIR
(F) CONTACT
TRACING
27.
TEXT
NEXT LECTURE
▸ Casescenarios
▸ preparation of EPIDEMIC CURVE
▸ Preparation of SPOT MAP
▸ Calculation of ATTACK RATE from a given data.
TEXT
RECAP
▸ IN THEPREVIOUS LECTURE
▸ PRINCIPLES OF PRIMARY HEALTH CARE.
▸ OUTBREAK CONTROL TEAM MEMBERS
31.
TEXT
OUTBREAK TEAM
MEMBERS
▸ ANEPIDEMIOLOGIST
▸ CLINICIAN
▸ MICROBIOLOGIST
▸ ENVIRONMENTAL HEALTH
OFFICER
▸ COMMUNICATION SPECIALIST
▸ DATA MANAGER
▸ ADMINISTRATIVE SUPPORT STAFF
32.
TEXT
RRT
In the eventof a suspected outbreak, the Rapid Response Teams (RRT)
-
a multidisciplinary team that looks into various aspects of an outbreak
is alerted.
RRT will be to investigate and confirm outbreak.
The members of RRT are regularly doing their work but, in the event of
an outbreak, come together to undertake a special function.
33.
TEXT
RRT
They should workin coordination with the Government health staff.
They will help and support health staff in management and control of
outbreak but the responsibility of implementing control measures
mainly rests with local health staff.
RRT should be formed at all levels of administrative system (district,
block, Panchayat).
The name, address and mobile phone number of RRT members should
be available at respective levels so that they can be alerted as soon as
possible.
36.
TEXT
CASE SCENARIO 1
Mr.X, Medical Officer of a primary health centre noticed increased
number of cases
with symptoms of fever, sore throat and cough during third week of
March. While taking detailed history one patient had a history of
international travel 2 weeks back from a place where some of his
friends also had similar illness.
In the next week, one of the tertiary care hospitals in the city reported
increased number of severe acute respiratory illness among admitted
patients and two of them died due to this.
As a Medical Officer or a member of a district health care team, how do
you investigate this and manage the situation?
37.
TEXT
CASE SCENARIO 2
Dr.X was appointed as Medical Officer of the Primary
Health Centre. One of his field staff reported three cases of
watery diarrhoea and dehydration (two mild and one
severe) in his field area and he referred them for admission
to the hospital.
As a health professional what do you think about this
episode and how do we proceed to investigate and control
the situation.
38.
TEXT
CASE SCENARIO 3
Dr.X was on casualty duty that day. Mr. Y, 49 years old, presented to Medicine
casualty
with high grade fever (3 days), retro-orbital pain, myalgia and rash.
While eliciting detailed history from the patient, he revealed that there was history of
fever and bodyache for his brother and brother’s wife one week back for which they
took treatment in a private hospital.
Mr. Y and his four brothers lived in nearby houses in the same compound (within 300
metres).
He took paracetamol on the first two days of fever thinking that he was feverish as he
walked in the rain the previous day.
As a health professional what do you think about this episode and how do we
proceed
to investigate and manage the situation.
39.
TEXT
CASE SCENARIO 4
Mr.A,17 years old, was brought to Medicine casualty with history of headache,
myalgia
and vomiting in the past 2 days. He reached home only 4 days back after a tour along
with 13 friends.
The day after he came home, he had mild fever and body ache. He
thought it might be due to tedious travel and took rest at home. But last night his
friend
phoned him and said that one of their friends was taken to hospital following fever,
vomiting and loss of consciousness.
As a health professional what do you think about this episode and how do we
proceed
to investigate and manage the situation.
40.
TEXT
CASE SCENARIO 1
Thisscenario suggests a possible
outbreak of a contagious respiratory
illness, potentially of pandemic
concern.
As a Medical Officer or a member of
the district healthcare team,
the approach to investigation and
management should follow
systematic outbreak investigation
steps while ensuring inter-sectoral
coordination as per the principles of
primary health care..
41.
TEXT
STEP 1: FORMATIONOF A RAPID
RESPONSE TEAM BY DISTRICT HEALTH
AUTHORITY
1) Medical Officer (PHC)- Leads local investigation
and response.
2) Epidemiologist- Analyses data, confirms
outbreaks, and tracks spread.
3) Microbiologist/Laboratory Personnel - Collects
and tests samples.
4) Public Health Nurse/Health Inspector - Conducts
community surveys and ensures preventive measures.
5) District Surveillance Officer (DSO)- Coordinates
reporting and response with state/national authorities.
6) Administrative Officer (from Local Government) -
Facilitates inter-sectoral coordination with municipal
authorities, police, and transport officials.
42.
TEXT
STEP 2: CASEDEFINITION & CASE
FINDING
1) Establish a working case definition
(e.g., fever + sore throat + cough + recent
travel/contact history).
2) Conduct active case search in hospitals,
community health centers, and primary
care clinics.
3) Contact tertiary care hospitals for
retrospective case review.
4) Enhance Integrated Disease
Surveillance Programme (IDSP) reporting
for real-time data collection.
43.
TEXT
STEP 3: CONFORMTHE
DIAGNOSIS
1) Collect throat/nasal swabs
from suspected cases and
send them for RT-PCR or
other diagnostic tests.
2) Confirm the causative
agent (e.g., Influenza, SARS-
CoV-2, or another novel
respiratory virus).
44.
TEXT
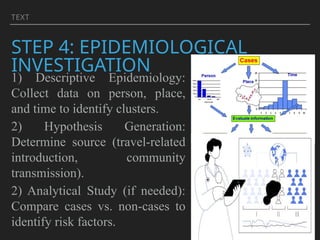
STEP 4: EPIDEMIOLOGICAL
INVESTIGATION
1)Descriptive Epidemiology:
Collect data on person, place,
and time to identify clusters.
2) Hypothesis Generation:
Determine source (travel-related
introduction, community
transmission).
2) Analytical Study (if needed):
Compare cases vs. non-cases to
identify risk factors.
45.
TEXT
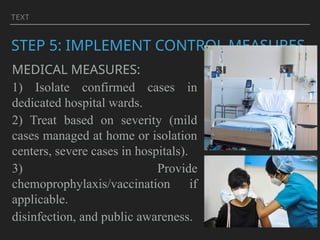
STEP 5: IMPLEMENTCONTROL MEASURES
MEDICAL MEASURES:
1) Isolate confirmed cases in
dedicated hospital wards.
2) Treat based on severity (mild
cases managed at home or isolation
centers, severe cases in hospitals).
3) Provide
chemoprophylaxis/vaccination if
applicable.
disinfection, and public awareness.
46.
TEXT
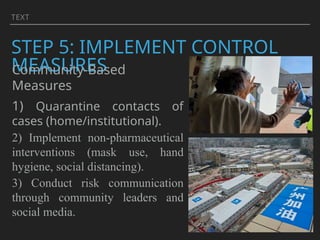
STEP 5: IMPLEMENTCONTROL
MEASURES
Community-Based
Measures
1) Quarantine contacts of
cases (home/institutional).
2) Implement non-pharmaceutical
interventions (mask use, hand
hygiene, social distancing).
3) Conduct risk communication
through community leaders and
social media.
47.
TEXT
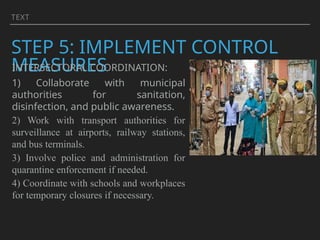
STEP 5: IMPLEMENTCONTROL
MEASURES
INTERSECTORAL COORDINATION:
1) Collaborate with municipal
authorities for sanitation,
disinfection, and public awareness.
2) Work with transport authorities for
surveillance at airports, railway stations,
and bus terminals.
3) Involve police and administration for
quarantine enforcement if needed.
4) Coordinate with schools and workplaces
for temporary closures if necessary.
48.
TEXT
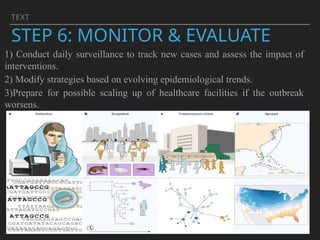
STEP 6: MONITOR& EVALUATE
1) Conduct daily surveillance to track new cases and assess the impact of
interventions.
2) Modify strategies based on evolving epidemiological trends.
3)Prepare for possible scaling up of healthcare facilities if the outbreak
worsens.
49.
TEXT
STEP 7: REPORTAND
COMMUNICATE FINDINGS
1) Report cases to
state/national
health authorities
(IDSP, ICMR,
MoHFW).
2) Conduct post-
outbreak analysis
to document
lessons learned and
improve future
response plans.






















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















